
Remember me




In CF-related advanced pulmonary disease, defined by an FEV1 lower than 40% of the predicted, ETI treatment, if indicated, is associated with rapid clinical improvement, often leading to suspension or withdrawal of the patient from the lung transplantation list. In an observational study, ETI administration for one to three months in 245 patients with advanced lung disease was associated with a mean increase in predicted FEV1 by 15.1%, which is consistent with our case, in addition to a substantial reduction in chronic oxygen therapy and non-invasive ventilation requirement [7]. Furthermore, this improvement is long-lasting, as demonstrated by another study, where among 65 patients eligible for a lung transplant, the improvement in FEV1 after ETI initiation remained stable after a mean follow-up of one year, allowing most individuals to be removed and remain off the transplant list [8].
Due to the possible risk of liver failure and, more frequently, an increase of transaminase and bilirubin, ETI treatment is currently not routinely indicated in individuals affected by CF with a previous liver transplantation. This typology of patients has not been included in clinical trials that evaluate safety and efficacy of ETI therapy.
A previous study reported that in a patient with cirrhosis and portal hypertension, ETI led to liver transplantation. Indeed, the drug’s pharmacokinetics implies several drug-to-drug interactions: the triple modulator is a substrate of CYP3A4, and ivacaftor also weakly inhibits P-glycoprotein, an enzyme that metabolizes several drugs, including immunosuppressants such as cyclosporine, everolimus, sirolimus and tacrolimus, thus elevating their serum concentrations. Therefore, ETI may cause further hepatotoxicity.
Our patient’s respiratory impairment was so severe that lung transplantation was considered the only reasonable option. However, she was not eligible for this treatment for psycho-social reasons due to poor compliance with treatments and therapies. On the other hand, she did not meet the criteria to start the triple modulator because she had previously received a hepatic transplant. We tried administering the triple modulator to improve her poor prognosis based on previous reports exploring the ETI regimen’s safety and tolerability in liver transplant patients with CF. Remarkably, several retrospective case series involving liver transplant individuals with an immunosuppressive regimen of drug therapy metabolized by P-glycoprotein showed that the ETI regimen is safe and leads to clinical benefits in lung function, quality of life and BMI. In these patients, a transient elevation in transaminase and bilirubin resolved in most cases after ETI dose reduction and elevations in serum concentration of tacrolimus were managed with dose adjustments of the immunosuppressive regimen [4,5,6].
During the one year of follow-up, our young patient maintained regular hepatic markers, with stable serum concentration of the immunosuppressants, and no dose modulation was required. Considering the clinical outcomes, she has experienced a significant improvement in respiratory function (with a stable increase of FEV1 of more than 12%), BMI and quality of life, with a remarkable change in her life perspective. These aspects have been also objectified by the relevant difference in scores obtained on the CFQR (Cystic Fibrosis Questionnaire-Revised), health-related quality of life questionnaire filled out by the patient before and after treatment (total average score of 60/100 and 78/100 points respectively).
Our case further indicates that ETI can be well tolerated in patients with previous liver transplantation. It represents a lifesaving drug for patients without alternatives, dramatically improving their quality of life. This report adds to the evidence suggesting that the clinical benefits of ETI in liver transplant patients overcome risks, which may be limited with a close drug monitoring of immunosuppressants serum levels and functional liver tests.
Further studies with a long-term follow-up are required to confirm the safety of this treatment in this specific group of patients.
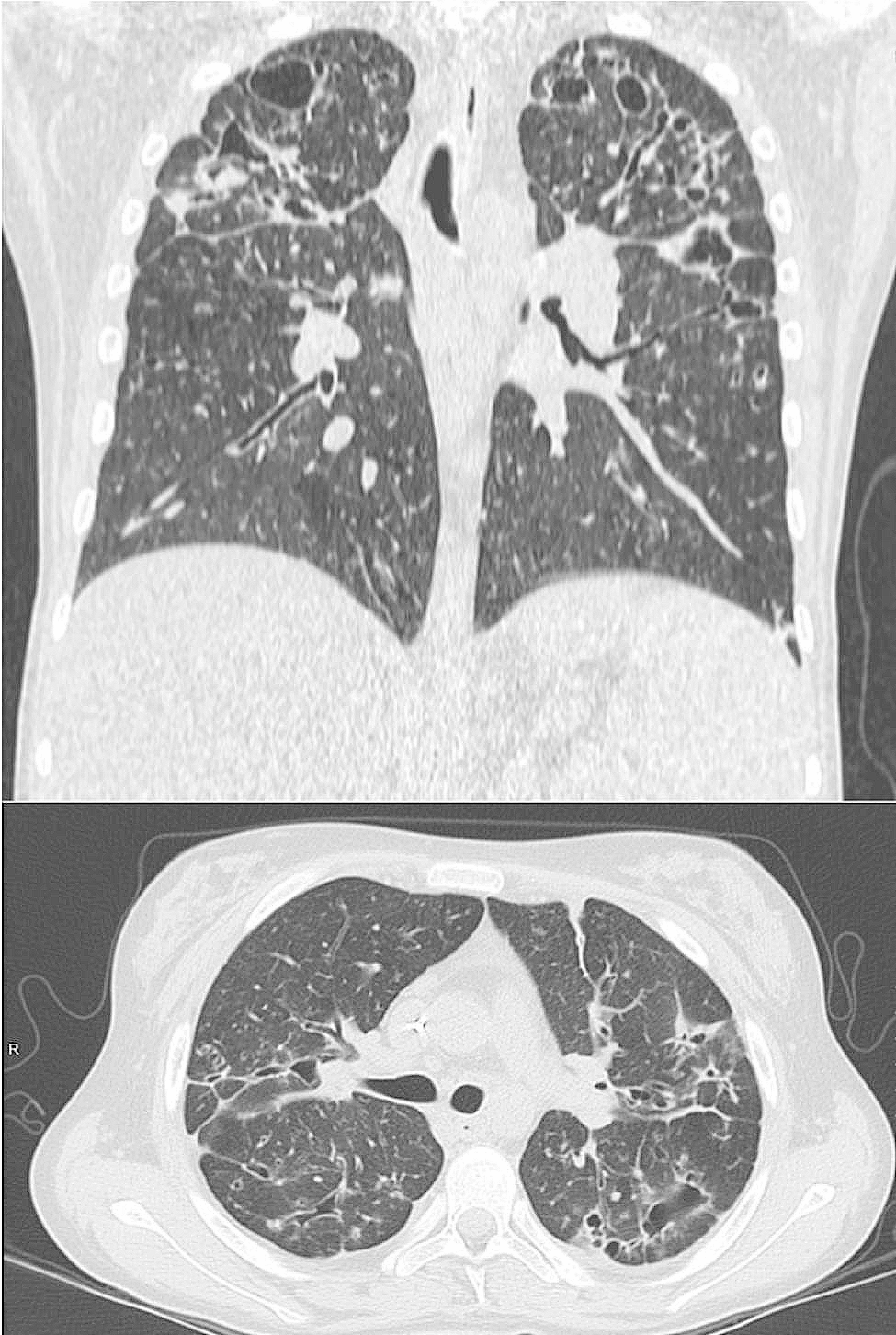
Fig. 1
Chest CT-scans show multiple giant apical bronchiectasis and a middle lobe syndrome
Comments (0)