Study Design
This retrospective cohort study used data from the DPC database. Data for patients matching the inclusion criteria were extracted from the database. Data for patients who met the exclusion criteria were then excluded. Patients were categorized into either the ACE or the CE cohort which were the experimental and control cohorts, respectively. Differences between the cohorts in terms of incidence of AEs were examined and further analyzed using survival analysis methods.
This study was conducted in compliance with the Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research Involving Human Subjects (Notification No. 1 of the Ministry of Education, Culture, Sports, Science and Technology/Ministry of Health, Labour and Welfare, dated February 28, 2017). The study was approved by an ethical review board (Non-Profit Organization MINS Institutional Review Board) and is registered in the UMIN Clinical Trials Registry (ID UMIN000041508). Informed consent was not required as this is a database study using anonymized data that are devoid of any patient-identifying information per the Japanese ethical guidelines.
Inclusion Criteria
Patients with a diagnosis of SCLC in their medical records were included. The C34 category (malignant neoplasm of bronchus and lung) of the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) was used to define SCLC. Patients with disease codes in category C34, excluding those considered not to be SCLC, were defined as eligible for this study. The excluded diseases are listed in Supplementary Table S1. Additionally, patients were required to have medical records prior to the observation period.
Exclusion Criteria
Patients who had been diagnosed with other comorbid malignant tumors during the data extraction period and those who had received chemotherapy for SCLC during the baseline period were excluded.
Data Source
A healthcare database owned by Medical Data Vision Co., Ltd. (MDV; Tokyo, Japan) was used as the data source. This database contains information from medical institutions that use the DPC payment system. Approximately 28,440,000 patients from 385 medical institutions were registered in the database at the time of the study.
Definitions
The ACE and CE cohorts were defined on the basis of the drugs prescribed in the month of the data extraction and the inclusion of SCLC (as defined in the inclusion criteria) in the records during this month. Drugs were defined using the Anatomical Therapeutic Chemical (ATC) classification system. The ATC codes for each drug are as follows: ACE cohort—L01XC32, atezolizumab; L01XA02, carboplatin; and L01CB01, etoposide. CE cohort—L01XA02, carboplatin and L01CB01, etoposide.
Data Extraction Period
For both cohorts, data from August 2019 (the month in which ACE combination therapy was approved in Japan for ED-SCLC) to March 2020 (the most recent data available for use) were used. A specific period was not determined for extracting the baseline data in this study. All data from before the start date of the observation period were used to extract the covariate information for the patients. As a side note, durvalumab, an immune checkpoint inhibitor treatment option like atezolizumab, was not approved in this period in Japan. In addition, patients without a baseline period were also included in the study, assuming that after the diagnosis of ED-SCLC in routine clinical practice, treatment would have started relatively quickly for most patients after their transfer to the medical institution included in the database. Any imbalance in the duration of the baseline periods between the cohorts was evaluated to avoid bias or confounding of the results.
First Day of Observation Period
The first day of the observation period was defined as the date of the earliest visit to a hospital when the SCLC diagnosis was recorded for the patient and a prescription for ACE or CE was provided.
Assessment of AEs
The incidence of the following 19 AEs was evaluated: interstitial lung disease (ILD), hepatic dysfunction, colitis/diarrhea, pancreatitis, type 1 diabetes, thyroid disease, adrenal disorder, hypopituitarism, meningitis/encephalitis, neuropathy, Guillain–Barré syndrome, myasthenia gravis, dermatopathy, renal dysfunction, myositis/rhabdomyolysis, myocarditis, febrile neutropenia, arthritis, and eye disorder. These AEs were defined on the basis of the ICD-10 codes corresponding to diseases in the health insurance claims extracted from the MDV database. Similarly, the treatments (i.e., ACE, CE, or others) were defined on the basis of the ATC codes. The ICD-10 and treatment codes are provided in Supplementary Tables S2 and S3.
For each of the 19 AE categories, clinically significant adverse events (CSAEs) were extracted and analyzed. Two definitions were used for the analysis of CSAEs and a separate analysis was performed using each definition: (1) if the patient was not prescribed ACE or CE by the planned date of prescription (43 days after the day on which ACE or CE was prescribed, immediately before the occurrence of the AE) after starting treatment for the AE, then the corresponding AE was considered a CSAE and (2) if the patient was hospitalized after an AE that met definition 1 and the main reason for the hospitalization was the AE, then the corresponding AE was considered a CSAE.
Statistical Analysis
The incidence of AEs was evaluated using incidence rates (cases per person-month), and differences between the ACE and CE cohorts were compared using incidence rate ratios.
The following covariates were adjusted using the inverse probability weighting (IPW) method [8]: age (< 71 or ≥ 71 years), sex, body mass index, presence of ILD before treatment, steroid use, activities of daily living score (100 or not), TNM classification 1 (T4 or not), and TNM classification 2 (M1 or not). Propensity scores were estimated using a logistic regression model with these covariates as the explanatory variables. On the basis of the propensity scores, the weighted population was obtained using the normalized stabilized weights.
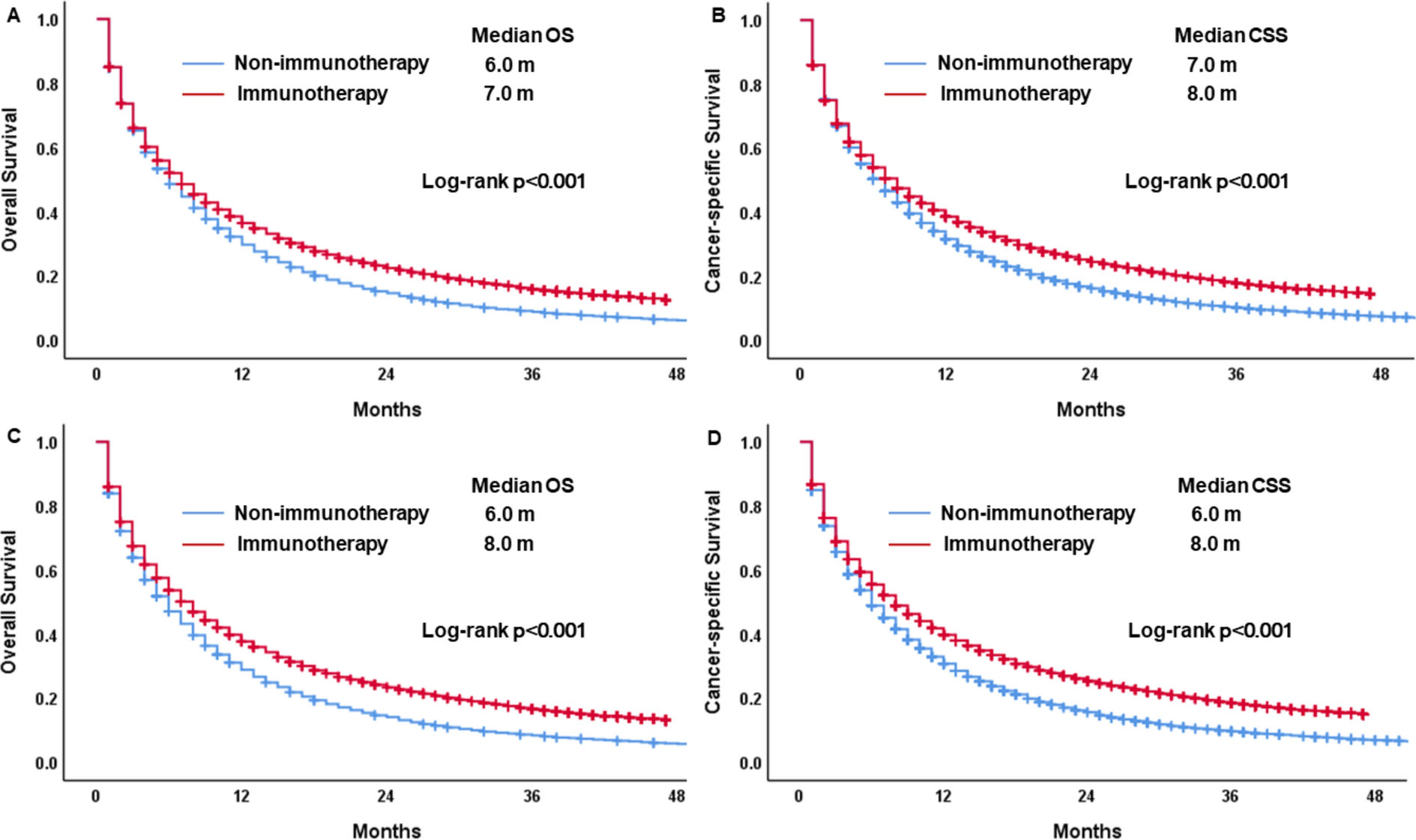
In addition to the adjusted incidence rates, adjusted Kaplan–Meier curves were generated, based on which adjusted restricted mean survival times (RMSTs) were derived [9] with truncation at 6 months. Results from two measures (i.e., incidence rate ratio and RMST difference) were used to demonstrate the robustness of the results.
Treatments for AEs
The number and proportion of patients who experienced AEs and received treatment for the AEs were analyzed. The analyzed treatments included drugs prescribed to treat the AEs, drugs categorized as L04 (immunosuppressants) in the ATC classification, and other drugs and medical procedures of clinical significance. Treatments administered in the same month as when the AE was documented were used for the analyses.



Comments (0)