
Remember me


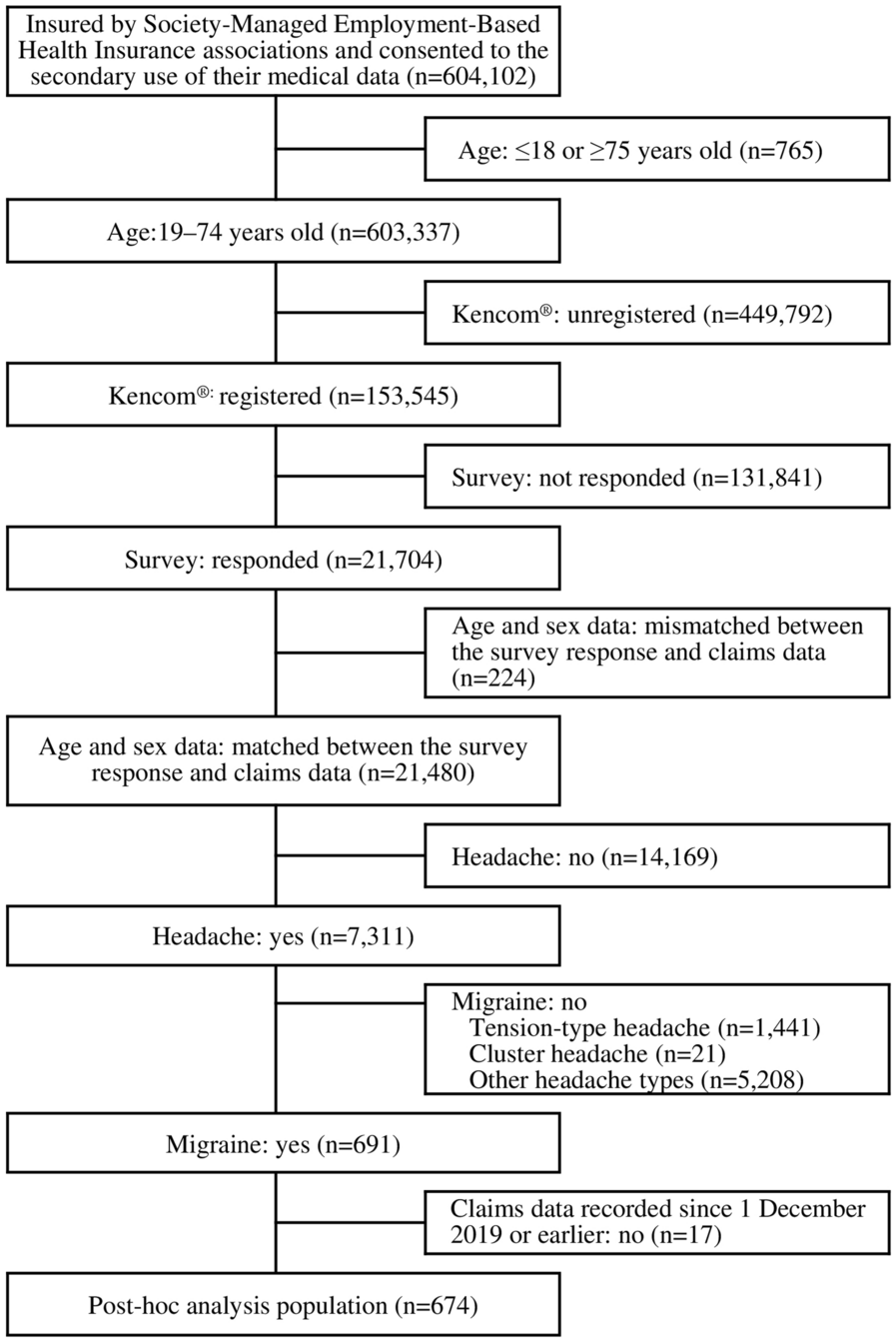

In total, 17,958 patients initiating at least one triple therapy were identified. The study included 3194 BGF initiators, 11,179 patients in the FF/UMEC/VI user cohort, and 5931 patients in the MITT user cohort. Out of the BGF initiators, 636 were in the BGF early adopter cohort, 401 of whom had BGF as the first triple therapy and 235 switched from another triple therapy; 2558 were in the contemporary BGF user cohort, 1466 of whom had BGF as the first triple therapy and 1092 switched from another triple therapy. Patient disposition is depicted in Fig. 2.
Fig. 2
Flowchart of study population. BGF budesonide/glycopyrronium/formoterol fumarate dihydrate, FF/UMEC/VI fluticasone furoate/umeclidinium, MITT multiple-inhaler triple therapy, TT triple therapy
Patient Demographic and Clinical CharacteristicsPatient demographics were generally similar across cohorts; mean (SD) age at index date was 73.7 (10.0) years in the early BGF adopter cohort, 73.1 (10.1) years in the contemporary BGF user cohort, 72.9 (9.9) years in the FF/UMEC/VI user cohort, and 72.0 (11.3) years in the MITT user cohort (Table 1). Use of the MDV database provided good coverage of the older population, especially those with severe health status [7]. There was a high proportion of male patients in each cohort; 74.4% in the early BGF adopters, 72.5% in the contemporary BGF users, 77.1% in the FF/UMEC/VI users, and 66.5% in the MITT users (Table 1). Consistent with the main cohorts, patient demographics were generally balanced across the BGF cohort subgroups (Supplementary Material, Table S2).
Table 1 Baseline demographic characteristics by cohortWhile clinical information is not readily obtainable in the MDV, data presented in Table 2 show that baseline clinical characteristics were similar across cohorts. Unspecified COPD was the most frequently occurring diagnosis code for all patients before initiating triple therapy (60.7–75.6% across cohorts), but 36.0–40.5% had diagnoses for chronic bronchitis and 29.4–32.7% had diagnoses of emphysema, though not mutually exclusive. Asthma + COPD was reported in 464 (73.0%) patients in the early BGF adopter cohort (221 [94.0%] of whom had switched to BGF from another triple therapy), 1898 (74.2%) in the contemporary BGF user cohort (975 [89.3%] of whom had switched to BGF from another triple therapy), 8457 (75.7%) in the FF/UMEC/VI user cohort, and 5013 (84.5%) in the MITT user cohort (Table 2 and Supplementary Material, Table S3). Of note, only 1063 (5.9%) had EOS data available. The mean (SD) EOS percentage per patient among the early BGF adopter and contemporary BGF user cohorts was 5.3% (6.9) and 3.3% (3.3), respectively, compared with 4.2% (5.1) and 3.7% (3.8) in the FF/UMEC/VI and MITT cohorts, respectively. Likewise, while data related to spirometry was limited, approximately 52.0% of patients had an indication that a test was performed.
Table 2 Baseline clinical characteristics by cohortMultimorbidityIn the 12-month pre-index period, the frequency of multimorbidity was comparable across cohorts, with over half of patients in all cohorts (52.4–56.9%) having a weighted ECI ≥ 5, and > 80% of patients having ≥ 1 ECI-related condition (Table 3). Cardiovascular diseases (including uncomplicated hypertension, congestive heart failure, cardiac arrythmias, and peripheral vascular disease) were among the most frequently observed, with similar rates across cohorts (Fig. 3). In the 12-month pre-index period, the frequency of multimorbidity was similar across BGF cohort subgroups compared with the main cohorts (Supplementary Material, Table S4).
Table 3 Baseline multimorbidity (reported in > 5% of any cohort) during the 12-month pre-index period by cohortFig. 3
Most frequently observed cardiovascular diseases during the 12-month pre-index period by cohort. BGF budesonide/glycopyrronium/formoterol fumarate dihydrate, FF/UMEC/VI fluticasone furoate/umeclidinium/vilanterol, MITT multiple-inhaler triple therapy
Prior Therapy (Maintenance and Non-maintenance) Treatment PatternsAlmost three quarters of patients across cohorts had some baseline maintenance treatment in the 12-month pre-index period. ICS/LABA dual therapy was the most common maintenance therapy across cohorts and was used by more than 38.0% of patients in every cohort (Fig. 4). Slightly more patients in the FF/UMEC/VI and MITT cohorts received ICS/LABA treatment (48.3% and 51.7%, respectively) compared with the BGF cohorts (38.2% and 40.9%, respectively), and more patients in the BGF cohorts had received LABA/LAMA treatment (31.1% and 26.0%, respectively) than in the MITT cohort (17.3%; Fig. 4). Approximately one-quarter of patients across cohorts had not received any maintenance treatment in the 12-month pre-index period.
Fig. 4
Maintenance therapy treatment patternsa during the 12-month pre-index period by cohort. aPatients within each cohort could have received more than one type of maintenance therapy in the 12-month index period and therefore percentages may exceed 100%. BGF budesonide/glycopyrronium/formoterol fumarate dihydrate, FF/UMEC/VI fluticasone furoate/umeclidinium/vilanterol, ICS inhaled corticosteroid, LABA long-acting β2-agonist, LAMA long-acting muscarinic antagonist, MITT multiple-inhaler triple therapy
In the early BGF adopter and contemporary BGF user cohorts, the most common COPD maintenance medication classes ≤ 90 days before initiation of BGF were ICS/LABA single-inhaler dual therapy (20.9% and 24.9%, respectively) and LABA/LAMA single-inhaler dual therapy (19.5% and 16.1%, respectively). At ≤ 90 days before initiation of BGF, over half of patients in the early BGF adopter and contemporary BGF user cohorts were using ≥ 1 COPD maintenance medication (56.0% and 55.6%, respectively). However, the number of days from the end of the previous maintenance treatment to BGF initiation was higher in the contemporary user cohort (mean, 41.7 [SD 25.2]; median, 35 [IQR 25; 56]) compared with the early BGF user cohort (mean, 34.7 [SD 24.7]; median, 28 [IQR 14; 56]).
Differences were observed in supplemental oxygen use for patients in the BGF cohorts versus the other cohorts. Oxygen therapy was dispensed in 12.9% of the early BGF adopter cohort, 12.7% of the contemporary BGF user cohort, 9.3% of the FF/UMEC/VI user cohort, and 6.5% of the MITT user cohort.
Treatment patterns with any respiratory antibiotic in the 12-month pre-index period were also similar across cohorts, with a slight trend for more antibiotic use in the early BGF adopter cohort; respiratory antibiotics were received by 54.7% of the early BGF adopter cohort, 47.1% of the contemporary BGF user cohort, 44.2% of the FF/UMEC/VI user cohort, and 50.2% of the MITT user cohort.
Non-maintenance therapy treatment patterns in the 12-month pre-index period were generally similar across BGF and MITT cohorts, with slightly lower proportions observed for the FF/UMEC/VI user cohort. Any rescue inhaler was used by 31.3% of the early BGF adopter cohort, 28.6% of the contemporary BGF user cohort, 27.6% of the FF/UMEC/VI user cohort, and 33.8% of the MITT user cohort. A short-acting β2-agonist (SABA) was used by 31.1%, 28.5%, 27.6%, and 33.7% of patients in the BGF early adopter, contemporary BGF, FF/UMEC/VI, and MITT cohorts, respectively, and a short-acting muscarinic antagonist (SAMA) was used by 0.5%, 0.3%, 0.2%, and 0.4% of patients in the BGF early adopter, contemporary BGF, FF/UMEC/VI, and MITT cohorts, respectively. There was no use of a SAMA/SABA combination in one device in any cohort. At least one prescription of OCS in the prior 12 months occurred among 26.6% of the early BGF adopter cohort, 24.1% of the contemporary BGF user cohort, 21.1% of the FF/UMEC/VI user cohort, and 26.2% of the MITT user cohort.
ExacerbationsThere was a trend towards a higher proportion of patients having experienced moderate/severe exacerbations, moderate exacerbations, or severe exacerbations during the 12-month baseline period in the BGF early adopter cohort compared with the other cohorts (Fig. 5). The mean (SD) number of moderate/severe COPD exacerbations before initiation of triple therapy was 0.3 (0.7) in the early BGF adopter cohort, 0.2 (0.7) in the contemporary BGF user cohort, and 0.2 (0.6) in both the FF/UMEC/VI and MITT user cohorts. The mean (SD) number of moderate COPD exacerbations or severe COPD exacerbations before initiation of triple therapy, respectively, was 0.2 (0.5) and 0.1 (0.5) in the early BGF adopter cohort, 0.1 (0.6) and 0.1 (0.3) in the contemporary BGF user cohort, and 0.1 (0.5) and 0.1 (0.3) in both the FF/UMEC/VI and MITT user cohorts. The proportion of patients with prior severe exacerbations across cohorts ranged from 5.3% to 8.8%. The percentage of patients with ≥ 1 moderate/severe exacerbation was 18.2% in the BGF early adopter cohort, 14.3% in the contemporary BGF user cohort, 13.1% in the FF/UMEC/VI user cohort, and 14.0% in the MITT user cohort. The distribution of the number of prior exacerbations during the 12-month pre-index baseline period by severity are presented in the Supplementary Materials (Table S5).
Fig. 5
Proportions of patients with moderate/severe exacerbations, moderate exacerbations, or severe exacerbations during the 12-month pre-index period by cohort. BGF budesonide/glycopyrronium/formoterol fumarate dihydrate, FF/UMEC/VI fluticasone furoate/umeclidinium/vilanterol, MITT multiple-inhaler triple therapy
Approximately twice as many patients who switched to BGF from another triple therapy (27.2% for the BGF early adopter cohort; 19.0% for the contemporary BGF user cohort) had a moderate or severe exacerbation than those who received BGF as their first triple therapy (13.0% for the BGF early adopter cohort; 10.8% for the contemporary BGF user cohort) in both the early adopters and contemporary cohorts, respectively (Supplementary Material, Table S3).
Healthcare Resource Utilization During the 12-Month Pre-index PeriodHospital Clinic Outpatient VisitsThe mean (SD) number of outpatient visits before initiation of triple therapy was 14.1 (19.1), 11.5 (11.1), 11.1 (11.7), and 11.0 (13.3) per patient for the BGF early adopter, contemporary BGF, FF/UMEC/VI, and MITT cohorts, respectively (Table 4). When grouped across specialties, most outpatient visits were observed for Respiratory/Pulmonology/Allergy specialties (64.2%, 67.8%, 64.7%, and 55.9% of patients in the BGF early adopter, contemporary BGF user, FF/UMEC/VI user, and MITT user cohorts, respectively). Cardiovascular-related visits were the third most frequently observed specialty outpatient visits (occurring in 18.7–22.8% of patients across cohorts) after Internal Medicine-related visits (occurring in 31.6–36.7% of patients across cohorts; Table 4).
Table 4 HCRU during the 12-month pre-index baseline period by cohortHospitalizationThe mean (SD) number of all-cause hospitalizations was 0.8 (1.2) per patient in the BGF early adopter cohort, 0.6 (1.1) per patient in the contemporary BGF user cohort, 0.6 (1.1) per patient in the FF/UMEC/VI user cohort, and 0.7 (1.1) per patient in the MITT user cohort. The mean (SD) length of stay was 12.1 (12.8), 12.8 (16.0), 10.9 (12.9), and 10.8 (12.5) days for the BGF early adopter, contemporary BGF user, FF/UMEC/VI user, and MITT user cohorts, respectively (Table 4). Overall 56–66% of hospital admissions were missing specific data on the ward of admission. Among the remaining 34–44% of patients with ≥ 1 hospitalization and available ward data, the most frequent wards of admission across cohorts included Internal Medicine (23.4–33.2%), Pulmonary Medicine (17.1–26.5%), Pulmonology (7.5–10.6%), and Cardiovascular Medicine (6.8–8.9%) (Supplementary Material, Table S6). A higher proportion of patients in the MITT user cohort reported ≥ 1 pneumonia-specific hospitalization compared to other cohorts (6.4%, 5.8%, 6.1%, and 7.4% in BGF early adopter, contemporary BGF user, FF/UMEC/VI user, and MITT user cohorts, respectively; Table 4).
Comments (0)