
Remember me


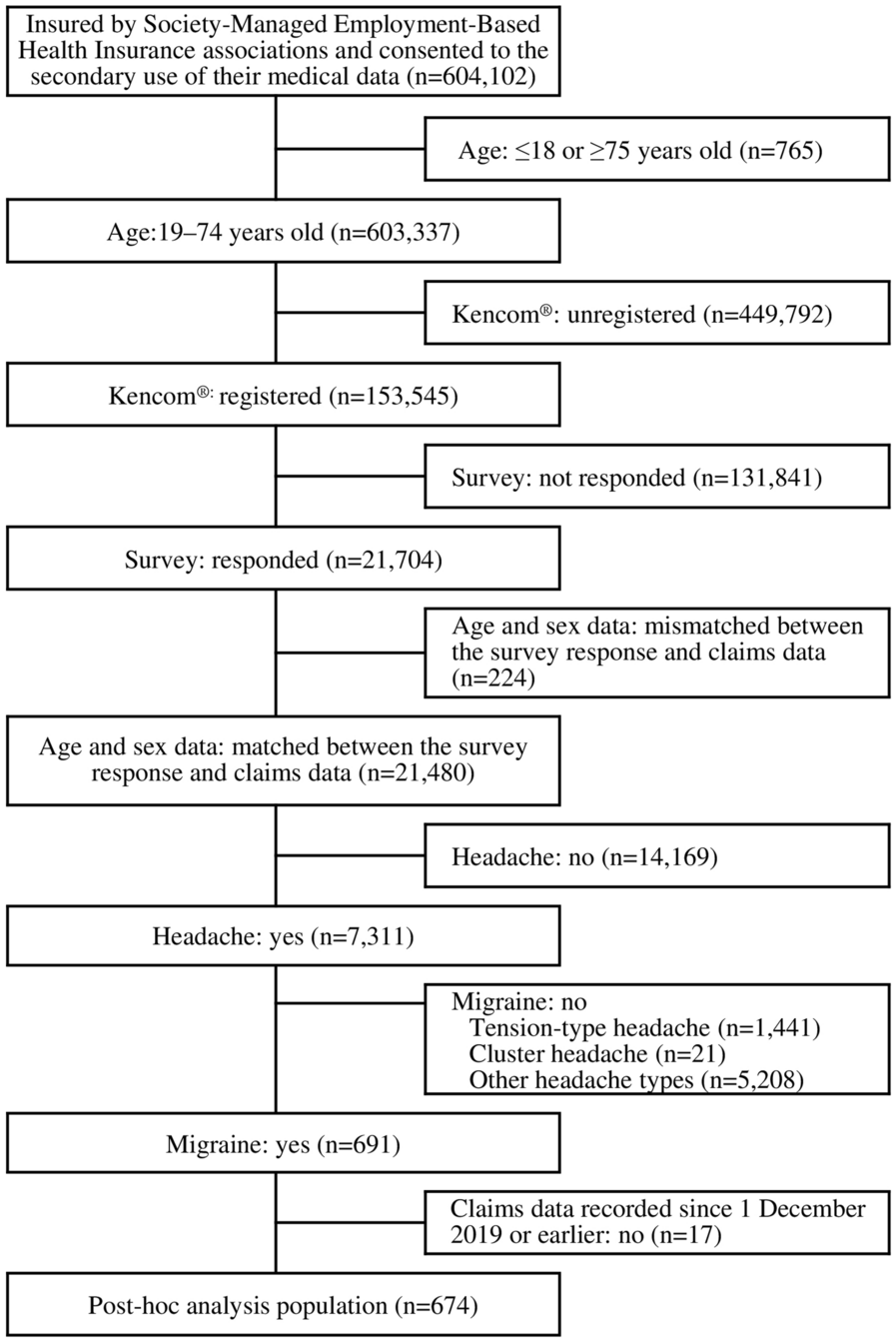

Of 164 patients (112 patients receiving lanadelumab and 52 patients not receiving lanadelumab) enrolled in EMPOWER across 25 sites in the USA and 5 sites in Canada, 112 patients receiving lanadelumab (19 newly treated, 93 established) were included in the safety set (Fig. 2). The FAS included 109 patients receiving lanadelumab (18 newly treated, 91 established). In patients newly treated with lanadelumab, LTP other than lanadelumab in the 6-month period before enrollment mainly comprised intravenous and subcutaneous pdC1INH (6 and 1 patients, respectively). Before enrollment, 1 patient fulfilled the criteria for the established patient subgroup (received ≥ 4 lanadelumab doses) but discontinued treatment because of pregnancy planning. After enrollment, 13 patients discontinued lanadelumab for reasons of adverse events related to treatment (1 newly treated, 1 established), lack of efficacy (3 established), patient’s/physician’s decision (2 established), issues with access to treatment including reimbursement/insurance (1 newly treated, 4 established), and pregnancy (1 established); these patients were censored from the primary analysis upon lanadelumab discontinuation but continued to contribute to other study outcomes.
Fig. 2
The EMPOWER sponsor ended the study earlier than planned and in agreement with the steering committee, based on consistency of the EMPOWER Study data with data from phase 3 lanadelumab trials. Before this, 4 of 19 patients newly treated with lanadelumab discontinued study participation for reasons including patient withdrawal due to issues with access to treatment (n = 1), site withdrawal from study (n = 1), loss to follow-up (n = 1), and patient withdrawal by their physician due to compliance issues (n = 1). Of 93 patients established on lanadelumab in the safety set, 19 discontinued study participation before the sponsor ended the study for reasons including site principal investigator leaving clinical practice (n = 7), patient’s decision (n = 3), site withdrawal from study (n = 2), physician’s decision (n = 2), loss to follow-up (n = 2), death unrelated to lanadelumab (n = 2 [COVID-19 infection, n = 1; traumatic brain injury, n = 1]), and withdrawal by parent/guardian (n = 1).
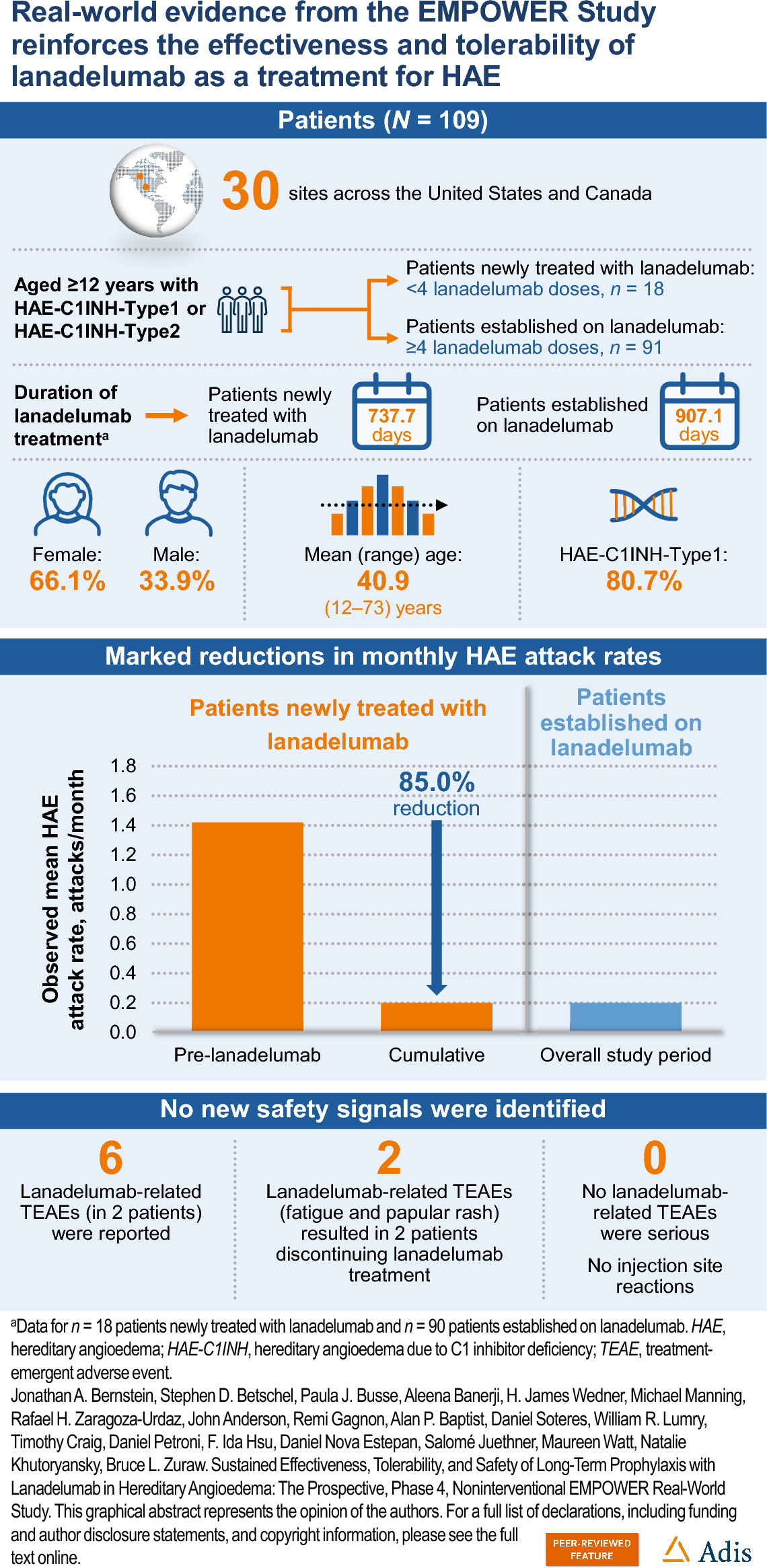
Patient Demographics and HAE CharacteristicsDemographics and baseline characteristics for all patients, patients newly treated with lanadelumab, and patients established on lanadelumab are summarized in Table 1. Patients were aged mean (SD) 40.9 (17.4) years at enrollment, with 12 (11.0%) aged < 18 years and 97 (89.0%) aged ≥ 18 years. Patients were mostly female (n = 72; 66.1%; 37 [33.9%] male) and white (n = 102; 93.6%), with Hispanic or Latino ethnicity reported for 13 (11.9%). Mean (SD) body mass index for patients was 30.8 (7.9) kg/m2. Most patients resided in the USA (n = 96; 88.1%) and the remainder (n = 13; 11.9%) in Canada.
Table 1 Demographics and baseline characteristics (full analysis set)Baseline HAE characteristics are shown in Table 2. Most patients had HAE-C1INH-Type1 (n = 88; 80.7%). Mean (SD) age at HAE diagnosis was 21.0 (14.8) years, with a mean (SD) time from symptom onset to diagnosis of 7.3 (12.8) years. Mean (SD) age at HAE diagnosis was slightly higher for patients established on lanadelumab (21.2 [15.0] years) versus patients newly treated with lanadelumab (19.6 [14.1] years). Among the patients included in the FAS, most (86/108 with available data; 79.6%) reported having a relative with HAE. Among the 86 patients who reported having a relative with HAE, more than three-quarters (66/86; 76.7%) had > 1 relative with HAE and over one-quarter (23/86; 26.7%) had ≥ 4 relatives with HAE. Most of the relatives with HAE were female (139/239 with available data; 58.2%).
Table 2 HAE characteristics (full analysis set)In the FAS, 77 patients (mean [SD] age, 41.4 [17.3] years; 66.2% female, 92.2% white; 84.4% HAE-C1INH-Type1) were on Q2W dosing at enrollment and remained on this dosing frequency throughout the study and 13 (mean [SD] age, 41.2 [21.2] years; 76.9% female, 100% white; 53.8% HAE-C1INH-Type1) were on Q4W dosing at enrollment and remained on this dosing frequency throughout the study. Eighteen patients (mean [SD] age, 35.1 [17.5] years; 61.1% female, 94.4% white; 77.8% HAE-C1INH-Type1) were on Q2W dosing at enrollment and later extended dosing intervals to Q4W (Table S2 in the Supplementary Material); product labeling allows extending dosing intervals if the patient is well controlled (e.g., attack free). Other dosing frequencies mainly included once every 3 weeks (every 20–21 days), except in 1 patient who received lanadelumab every 6 weeks (every 42 days). Lanadelumab dosing throughout the study in the overall EMPOWER population is summarized in Fig. S1 in the Supplementary Material.
HAE Attack RatePatients Newly Treated with LanadelumabOf 18 patients newly treated with lanadelumab in the FAS, 16 patients initiated lanadelumab after enrollment and 2 patients received lanadelumab before enrollment (1 and 3 doses). Mean (SD) duration of lanadelumab treatment during the study was 737.7 (374.5) days for patients newly treated with lanadelumab. At the end of study data collection, 16 patients newly treated with lanadelumab remained on lanadelumab. Among patients newly treated with lanadelumab, mean (SD) numbers of HAE attacks observed over time (mean [SD]) were 10.3 (12.9) over 360.5 (273.5) days (pre-lanadelumab initiation), 0.9 (1.3) over 67.9 (9.0) days (early state), 2.9 (6.2) over 522.3 (293.9) days (steady state), and 3.7 (6.8) over 561.2 (314.2) days (cumulative). One patient initiated lanadelumab within 50 days of study completion and therefore could not reach steady state before their last visit; thus, early-state (first 69 days of lanadelumab treatment) and cumulative period post-lanadelumab initiation analyses include data from 18 patients and steady-state analyses (day 70 onward) include data from 17 patients.
Mean observed HAE attack rate decreased from 1.42 (median, 0.39) attacks/month pre-lanadelumab to 0.20 (median, 0.10) attacks/month (IRR, 0.15) during the cumulative period post-lanadelumab initiation (Fig. 3). During the early-state period, mean attack rate was 0.41 (median, 0.43) attacks/month (IRR, 0.30), and during the steady-state period, mean attack rate was 0.21 (median, 0.00) attacks/month (IRR, 0.13). In patients newly treated with lanadelumab, the adjusted model-estimated mean HAE attack rate (attacks/month) decreased from 1.42 pre-lanadelumab to 0.17 during the cumulative period (IRR, 0.10) (Fig. 4). The sensitivity analysis was supportive of the primary statistical analysis: mean adjusted model-estimated attack rate was 0.39 and 0.14 during the early- and steady-state periods, respectively. Among patients newly treated with lanadelumab who experienced HAE attacks after treatment initiation, the frequency and severity of attacks varied, but most were mild or moderate in severity (Table S3a in the Supplementary Material). The most frequently reported concomitant HAE medication used by patients newly treated with lanadelumab during the treatment period was pdC1INH (Table S4 in the Supplementary Material).
Fig. 3
Mean observed HAE attack rates before and after lanadelumab initiation (full analysis set). Median observed HAE attack rates (attacks/month) in patients newly treated with lanadelumab at enrollment were 0.39 pre-lanadelumab and 0.10 in the cumulative period; and 0.06 attacks/month during the overall study period in patients established on lanadelumab at enrollment. CI confidence interval, HAE hereditary angioedema, IRR incidence rate ratio
Fig. 4
Mean adjusteda model-estimated HAE attack rates before and after lanadelumab initiation in patients newly treated with lanadelumab at enrollment (full analysis set; as treated). aModel adjusted for sex and age at lanadelumab initiation. CI confidence interval, HAE hereditary angioedema, IRR incidence rate ratio
In patients newly treated with lanadelumab, among the 4 with available data who received Q2W dosing at lanadelumab initiation and extended dosing intervals to Q4W, the mean HAE attack number decreased from 2.3 (median, 1.0) attacks per patient in the pre-lanadelumab period to 0.5 (median, 0.0) during the Q2W period, 0.0 (median, 0.0) during the Q4W period, and was 0.5 (median, 0.0) overall during the cumulative post-lanadelumab period (Table 3). Observed mean attack rate (attacks/month; 95% CI) was 0.37 (− 0.49, 1.22) for the pre-lanadelumab period and 0.04 (− 0.09, 0.17), 0.00 (–, –), and 0.03 (− 0.07, 0.14) for the Q2W, Q4W, and cumulative periods, respectively. For 14 patients newly treated with lanadelumab who received Q2W dosing at enrollment and remained on this dosing frequency throughout the study, the mean HAE attack number per patient was 12.6 (median, 6.0) in the pre-lanadelumab period and decreased to 4.6 (median, 1.0) in the cumulative post-lanadelumab period. Observed mean attack rate (attacks/month; 95% CI) was 1.72 (0.35–3.09) in the pre-lanadelumab period and decreased to 0.25 (0.02–0.48) in the cumulative period (Table 3).
Table 3 Observed HAE attack rate comparison by lanadelumab Q2W and Q4W (full analysis set)Patients Established on LanadelumabMean (SD) duration of lanadelumab treatment during the study was 907.1 (469.3) days for patients established on lanadelumab. At the end of study data collection, 79 patients established on lanadelumab at enrollment remained on lanadelumab. During the overall study period, patients established on lanadelumab had a mean (SD) of 4.2 (8.5) HAE attacks over a mean (SD) of 801.8 (319.5) days. The observed mean (95% CI) monthly attack rate was 0.20 (0.1, 0.3) attacks/month (median, 0.06) (Fig. 3). Similar to patients newly treated with lanadelumab, the frequency and severity of HAE attacks experienced by each established patient varied. Icatibant and pdC1INH were used by 47.3% (n = 43/91) and 13.2% (n = 12/91) of patients established on lanadelumab, respectively, for on-demand treatment of HAE attacks during the treatment period (Tables S3b and S4 in the Supplementary Material). Most HAE attacks were mild or moderate in severity (Table S3b in the Supplementary Material).
In the patients established on lanadelumab, among the 14 with available data who received Q2W dosing at enrollment and extended dosing intervals to Q4W, the mean HAE attack number per patient was 0.1 (median, 0.0) in the Q2W dosing period and 0.3 (median, 0.0) in the Q4W dosing period. HAE attack rate (attacks/month; 95% CI) changed from 0.01 (− 0.00, 0.02) attacks/month in the Q2W period to 0.02 (− 0.00, 0.05) during the Q4W period, and was overall 0.04 (0.00–0.07) during the cumulative post-lanadelumab period (Table 3). For 60 patients established on lanadelumab who received Q2W dosing at enrollment and remained on this dosing frequency throughout the study, the mean HAE attack number per patient was 4.6 (median, 2.0) and HAE attack rate (attacks/month; 95% CI) was 0.25 (0.11–0.39) attacks/month in the cumulative post-lanadelumab period (Table 3). Among 12 patients established on lanadelumab who received Q4W dosing at enrollment and remained on this dosing frequency throughout the study, the mean HAE attack number per patient was 3.1 (median, 0.5) and HAE attack rate (attacks/month; 95% CI) was 0.09 (− 0.01, 0.19) in the cumulative post-lanadelumab period (Table 3).
SafetyIn total, 58/112 patients in the safety analysis set reported 154 TEAEs. Of these 154 TEAEs, 6 (in 2 patients) were classified as related to lanadelumab (fatigue [n = 3], tachycardia [n = 2], and papular rash [n = 1]). None of the 6 lanadelumab-related TEAEs were considered serious. Of patients with lanadelumab-related adverse events (AEs), 1 newly treated patient and 1 patient established on lanadelumab at enrollment discontinued lanadelumab because of lanadelumab-related AEs (papular rash and fatigue, respectively). Among patients in the overall safety set, infections and infestations were the most frequent (43 events in 34 patients) TEAE by Medical Dictionary for Regulatory Activities System Organ Class, followed by gastrointestinal disorders (14 events in 10 patients) and general disorders and administration site conditions (11 events in 6 patients). There were no reports of lanadelumab-related injection site reactions. TEAEs were mostly mild (66/154) or moderate (79/154) in severity, with 7 classified as severe. Most TEAEs were nonserious (146/154), with 8 considered serious.
Of 19 patients newly treated with lanadelumab in the safety analysis set, 7 reported a total of 18 TEAEs. In the first 30 days of lanadelumab treatment, 1 patient reported 4 (22.2%) TEAEs (3 mild and 1 moderate in severity, all nonserious; 3 were considered related to lanadelumab). Between 30 and 90 days of lanadelumab treatment, 2 patients reported 4 (22.2%) TEAEs (2 mild and 2 moderate in severity, all nonserious; 2 were considered related to lanadelumab). No TEAEs were reported between 90 and 120 days of lanadelumab treatment. After 120 days of lanadelumab treatment, 6 patients reported 10 (55.6%) TEAEs (5 mild and 5 moderate in severity, all nonserious; none were considered related to lanadelumab).
Comments (0)