
Remember me



This was a post hoc analysis of an observational study that used combined cross-sectional online survey data and medical claims data. The methodologies used have been detailed elsewhere [12].
Briefly, we used preexisting anonymized data provided by DeSC Healthcare Inc. (DeSC). The data comprised online survey response data and linked health insurance medical claims data of multiple Society-Managed Employment-Based Health Insurance associations, one of the public employment-based health insurance plans in Japan. DeSC also developed a health application service, known as kencom®, through which online surveys were provided to the application users insured by the health insurers that consented to the secondary use of the data under the contract with DeSC.
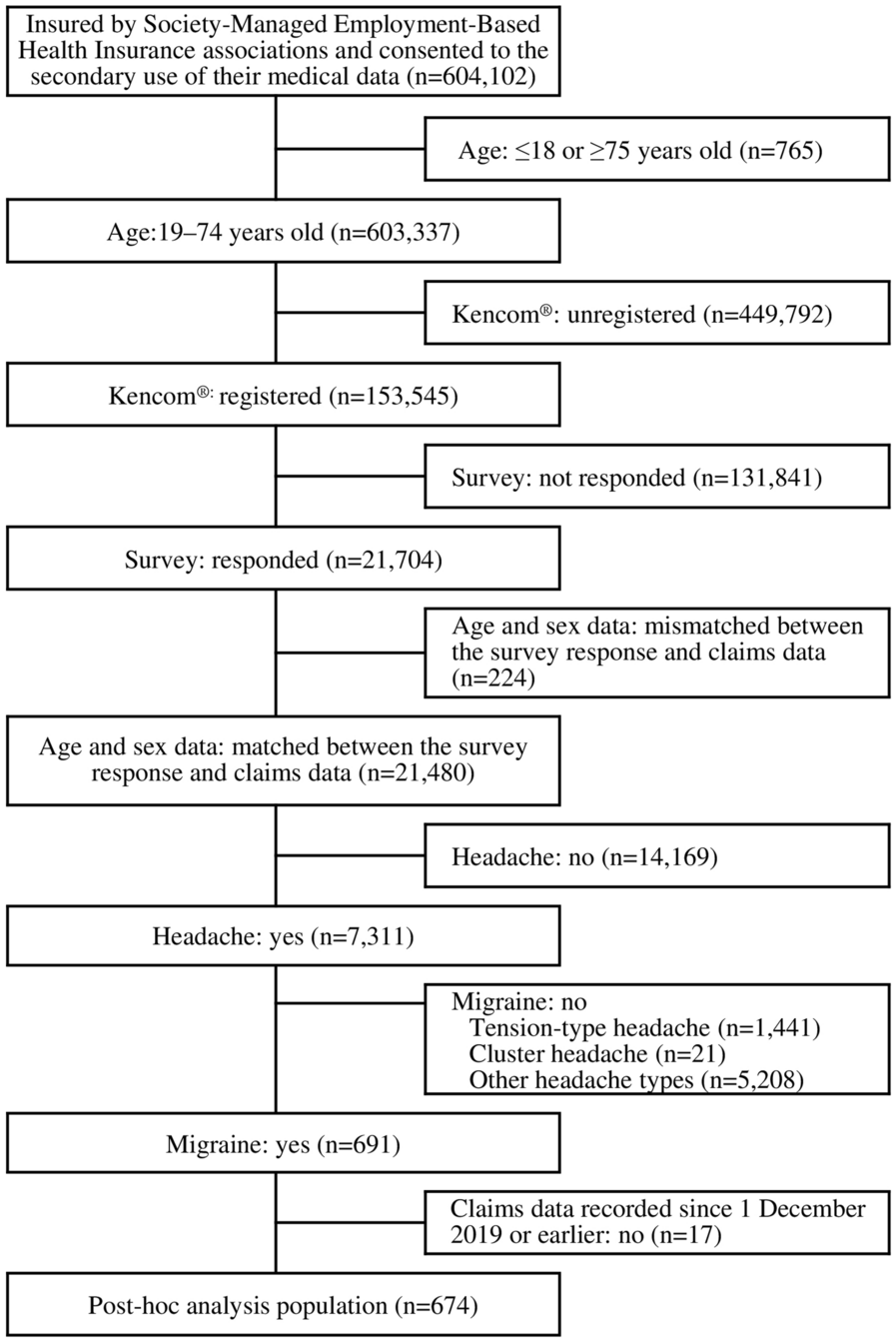
The survey data for this study were derived from a survey conducted from 1 to 30 November, 2020. kencom® users aged 19 to 74 years insured by Society-Managed Employment-Based Health Insurance associations who had consented to the secondary use of their medical data (Fig. 1) were eligible for the survey, irrespective of having headaches or not. Of 153,545 eligible kencom® users, 21,704 responded to the survey (response rate 14.1%). Among them, the medical claims data recorded during the claims data period from 1 December 2019 to 30 November 2020 were extracted from the database. To reduce the risk of including response data with a high probability of misclassification, the analysis population of the original study included only those whose sex and age information were the same between the survey response data and claims data that had been linked and anonymized before the study was conducted.
Fig. 1
This post hoc analysis focused on respondents with migraine from the analysis population of the original study. Migraine was defined on the basis of survey responses to the questions about headaches in the past 30 days as follows: (1) episodes lasting for half a day to 2–3 days; (2) unilateral pain; (3) throbbing or pulsating pain, and/or pounding pain; (4) pain worsened as a result of activities and/or was better when staying still; (5) associated with nausea or vomiting, and/or a combination of photophobia and phonophobia; and (6) moderate to extreme pain. These responses corresponded to the criteria of the International Classification of Headache Disorders, 3rd edition (ICHD-3); it should be noted, however, that the identification of migraine in this study relied on self-response data rather than physician assessment. Probable migraine, defined as a case that satisfied five of the above six criteria, was included as a migraine. We also assessed the burden of migraine relative to headache frequency in the same study population [13].
Ethical ApprovalWe utilized only a preexisting anonymously processed database developed and managed by DeSC. Originally, upon database construction, DeSC offered insured individuals the option to opt out of the provision of their medical data. Moreover, before proceeding to the survey questions, the kencom® application explained that the response data would be anonymized and provided to a third party, and proceeding to the questions would serve as consent for the use of their response data. These claims and survey data were linked and then anonymized by the DeSC in such a way that it was not possible to identify individuals and provided to the study investigators. Informed consent was not required for studies that used de-identified anonymized data. Therefore, no new individual consent was obtained for the use of the data in this study. The study protocol was approved by the Ethics Committee of the Research Institute of Healthcare Data Science (Approval no. RI220622; registration ID UMIN000050349) and was conducted in accordance with the Declaration of Helsinki (revised October 2013) by the World Medical Association and the Ethical Guidelines for Medical Research Involving Human Subjects. The authors had full access to the study data.
Respondents’ CharacteristicsRespondents’ demographic, socioeconomic, and clinical characteristics, including sex (claims data), age (claims data), employment status, annual household income, number of days with headaches in the past 30 days, and years lived with headaches, were extracted from survey responses (unless otherwise stated).
We assessed the comorbidities among the patients with migraine listed in the guidelines issued by the Japanese Society of Neurology, Japanese Headache Society, and Japanese Society of Neurological Therapeutics [5]. These comorbidities were identified on the basis of two or more medical claim records of the following International Classification of Diseases 10th revision (ICD-10) codes during the claims data period: epilepsy (ICD-10 codes G40, G41), cerebrovascular disorders (I60–I69), hypertension (I10–I15), cardiovascular disorders (I20–I52), gastrointestinal disorders (K20–K93), schizophrenia (F20), depression (F32,F33), anxiety disorders (F40, F41), somatoform disorders (F45), sleep disorder (G47), asthma (J45, J46), allergy (J30, L23, J450, K522, L500, T784), and autoimmune disorders (codes listed in Supplementary Material, Table S1). The Charlson Comorbidity Index was calculated as the total weight of the corresponding ICD-10 codes recorded twice or more during the claims data period [14].
OutcomesMSQMSQ was assessed using the MSQ Questionnaire version 2.1 [15,16,17] and data were extracted from the survey. The MSQ Questionnaire assesses the impact of migraine on the QOL of patients over the past 4 weeks in three domains: role function-restrictive (RR), role function-preventive (RP), and emotional function (EF) [16]. The RR and RP domains measure the extent to which migraine restricts (RR) and prevents (RP) work and daily and social activities on seven and four items, respectively. The EF domain measures emotional reactions associated with migraine using three items. Each question was rated on 6-point Likert scale (1, never to 6, all the time) and converted to domain scores ranging from 0 to 100, with higher scores indicating a better MSQ.
WPAIWork productivity and activity impairment (WPAI) were measured using the WPAI Questionnaire-General Health [18] and data were extracted from the survey. The questionnaire assessed the degree of loss in work productivity and daily activities over the past 7 days by yielding four scores: absenteeism, presenteeism, overall work impairment (OWI), and activity impairment (AI). The absenteeism score was calculated as the percentage of work hours missed based on the number of hours the respondents were absent from work due to their health problems and the number of hours that they worked. Presenteeism and AI scores were expressed as a percentage of the respondents’ ratings of the magnitude of the impact of their health problems on their work productivity and daily activities outside work, respectively, on an 11-point Likert scale: 0, no problem to 10, completely prevented. The OWI score was calculated as the total percentage of missed working hours and hours worked with impaired productivity. Higher scores indicate greater impairment in the productivity of work and daily activities.
Statistical AnalysisOf the 691 respondents with migraine who were included in the original analysis [12], we included those whose claims data had been recorded since 1 December 2019, or earlier, i.e., having claims data of the last 1 year or more from the survey, in this post hoc analysis (Fig. 1). We described the respondent characteristics by summarizing the categorical data with numbers and percentages and continuous data with mean (standard deviation [SD]) and median (first quartile [Q1], third quartile [Q3]).
MSQ scores were summarized as the mean (SD) for each subgroup of comorbidities. The assumption of normal distribution was verified using a distribution based on the histogram. For a skewed distribution, with many patients scoring 0, the WPAI score was summarized as the mean (SD) and median (Q1, Q3). To explore the association between MSQ and comorbidities coexisting with migraine, we compared MSQ scores using analysis of covariance (ANCOVA), with MSQ domain scores as outcomes and each comorbidity (presence vs absence, regardless of the number of comorbidities) as explanatory variables, adjusted for the following covariates: age, sex, and number of headache days in the past 30 days (monthly headache days). After adjusting for the same covariates, the association between the MSQ and the number of comorbidities was explored using ANCOVA, with the number of comorbidities (1, or ≥ 2 vs 0) as an explanatory variable. The adjusted differences in mean MSQ domain scores and their 95% confidence intervals (CI) between the subgroups of respondents with and without each comorbidity were estimated.
The association between the WPAI and comorbidities coexisting with migraine was explored using a logistic regression model. As noted earlier, because many respondents scored 0 on the WPAI, we dichotomized each WPAI score as 0 or above 0. The model set a WPAI domain score > 0 as an outcome and the presence or absence of each comorbidity (regardless of the number of comorbidities) or the number of comorbidities (1, or ≥ 2 vs 0) as explanatory variables, adjusted for age, sex, and monthly headache days. For each comorbidity, the odds ratios (OR) and 95% CI were calculated.
Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). No missing data were imputed. Statistical significance was set at p < 0.05 (two-tailed). As this analysis was exploratory, no statistical power calculation was conducted prior to the study. The sample size was based on data available from the DeSC database. The multiplicity of statistical testing was not adjusted, and the statistical test results should not be interpreted as confirmatory.
Comments (0)