
Remember me


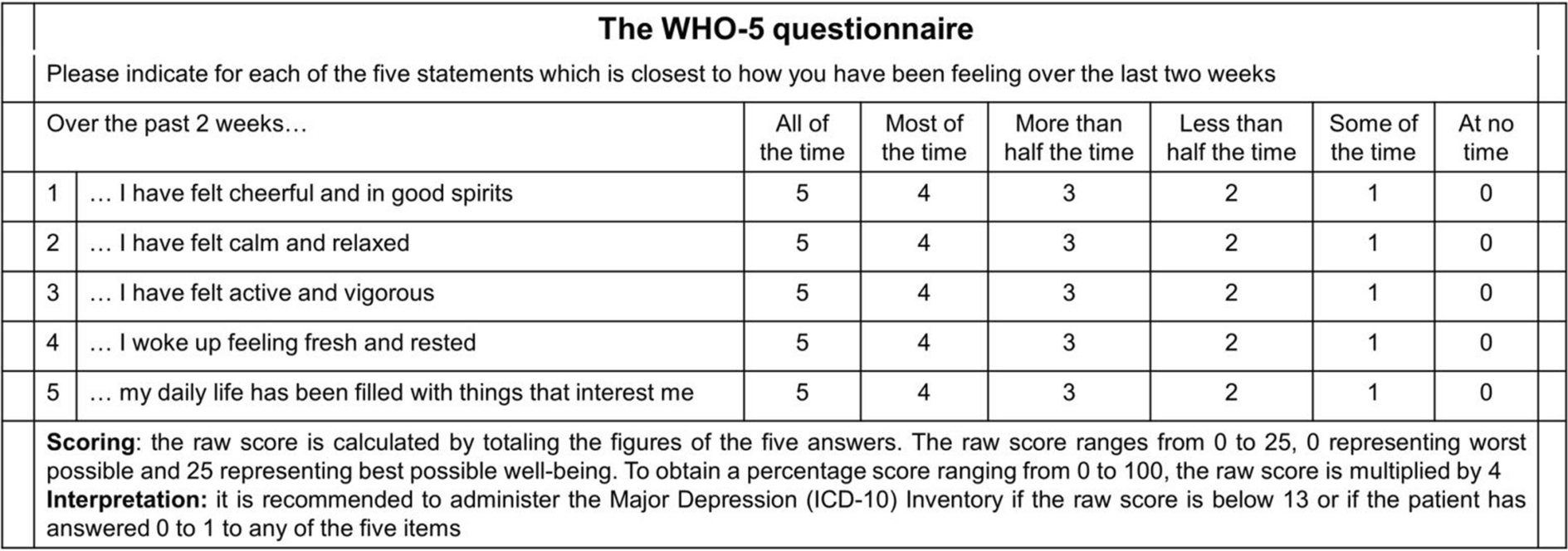

It is ideal to report the mean score and SD of the WHO-5 questionnaire in the population under study. In addition, in the case of an intervention, the ultimate goal should be to reach a WHO-5 score of the general population [24]. However, the mean score can also be complemented by the percentage of patients with impaired well-being or psychological distress (WHO-5 ≤ 50) and with possible clinical symptoms of depression (WHO-5 ≤ 28) [13].
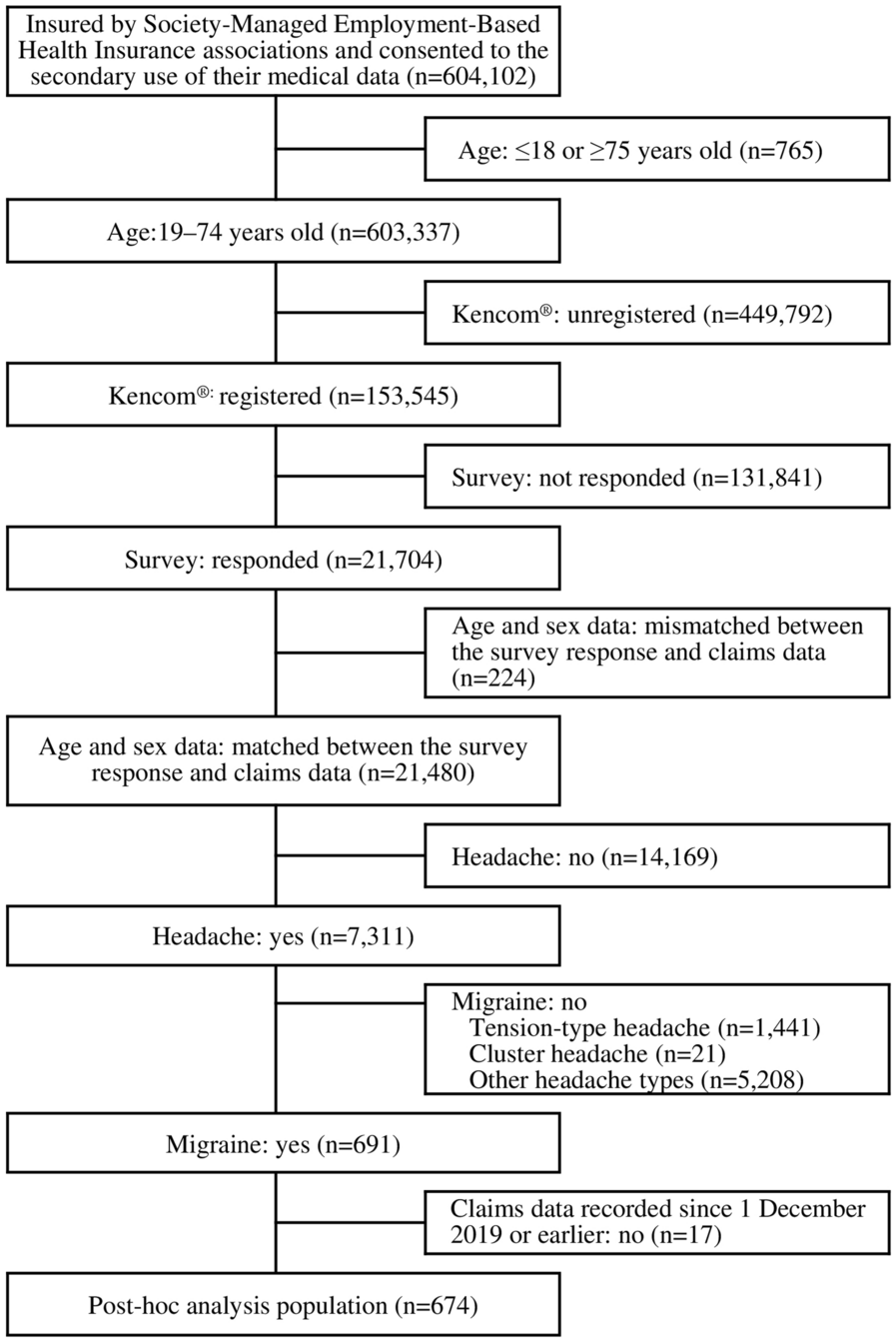
From the initial 1675 papers screened, 552 were included in this review (Fig. 2). Table 1 shows the different disease groups that implemented the WHO-5 questionnaire to measure well-being. The groups with the most publications refer to the COVID-19 pandemic (n = 161, 29.2%) followed by the group of mental, behavioral, or neurodevelopmental disorders (n = 141, 25.6%), with 45 on clinical depression and 96 in other mental disorders. The third most frequent disease area was the group of endocrine, nutritional, and metabolic diseases (n = 120, 21.7%).
Table 1 Use of the World Health Organization-Five Well-Being Index (WHO-5) questionnaire across disease areasMental, Behavioral, or Neurodevelopmental DisordersSince the WHO-5 questionnaire assesses psychological well-being, it is unsurprising that, until the COVID-19 pandemic, it was most frequently used in this area. However, the WHO-5 has been used for several other mental disorders, discussed below (Table 1; Table S1). When pooled together, the average WHO-5 score was 32.9 ± 0.2, indicating a well-being impairment in patients with mental disorders. However, when the conditions were analyzed separately, a disparity of results was observed. The ICD-11 classification was used to report the effect of WHO-5 in the different disorders [25].
Clinical DepressionAlthough the WHO-5 was developed as a screening tool for subjective well-being, 45 studies used the WHO-5 in patients with clinical depression (Table S2). As expected, the score was remarkably low, with an average of 26.9 ± 0.1. This score dropped to 22.3 ± 0.1 when only the 23 studies with patients diagnosed with major depressive disorder were included.
Most of these studies (n = 28) aimed to evaluate the effect of different kinds of intervention [anti-depressive treatment (n = 22), support-training programs (n = 8), changes in lifestyle (n = 4), or other interventions (n = 3)]. Although not all reported the WHO-5 score after the intervention, the vast majority mentioned a significant increase in the score. In the rest, authors aimed to test the reliability and correlation of WHO-5 with other well-established scales for measuring depression (MDI and/or PHQ-9).
Pooled data from 3530 outpatients with major depressive disorder enrolled in ten desvenlafaxine clinical trials aimed to explore the relationship between assessments of functional impairment, emotional well-being, and depression symptoms [26]. The study determined that a 2.5-point difference in the 25 points WHO-5 score between active treatment and placebo was clinically relevant in relation to improvements in depressive symptoms.
Neurocognitive DisordersDementia is not a specific disease but is rather a general term for the impaired ability to remember, think, or make decisions that interferes with doing everyday activities. The impairments of cognitive function are commonly accompanied, and occasionally preceded, by deterioration in emotional control, social behavior, or motivation. However, here only one study reported the WHO-5 in patients with mild-to-moderate dementia, with a mean score of 67.2 ± 20.5, similar to the general population. This score could be explained by the mild severity of the disease or by the fact that some patients with dementia are not aware of their cognitive decline. It is interesting to note that dementia strongly impacts the caregivers, with an average WHO-5 of 43.4 ± 0.3 in five studies including caregivers of older people with cognitive impairment or dementia.
Disorders Due to Substance Use or Addictive BehaviorsThis block contains a wide variety of disorders that differ in severity and clinical form, but are all attributable to the use of one or more psychoactive substances, which may or may not have been medically prescribed [27].
Regarding the use of drugs, there is a clear differentiation between studies assessing the sporadic use of drugs for recreational purposes and those studies in patients with a serious addiction. Thus, the two studies that evaluated the use of recreational drugs (i.e., methamphetamine, mephedrone, ketamine, or similar) without reporting addiction showed a good well-being, similar to the general population. In contrast, addiction to drugs (n = 3), alcohol (n = 3) or gambling (n = 1) seems to be highly associated with psychological distress (WHO-5 score of 46.2 ± 1.5), although the number of studies is limited to draw conclusions.
Schizophrenia or Other Primary Psychotic DisordersSchizophrenic disorders are characterized in general by fundamental and characteristic distortions of thinking and perception and an affect that is inappropriate or blunted.
WHO-5 was reported in two studies. One of them, is a real-world study including 242 predominantly symptomatically stable patients with diagnosis of schizophrenia under treatment but with serious impairment in functioning. One of the aims of the study was to evaluate the effect on well-being of aripiprazole once monthly, a novel long-acting injectable medicine that improved the functioning and QoL of the patients. After 28 weeks, the WHO-5 score significantly improved from 42.4 ± 22.4 (baseline) to 61.6 ± 10.8 [28]. Again, the use of the WHO-5 questionnaire demonstrated that uncontrolled disorders severely affect people’s well-being, and that appropriate treatment can restore it.
Mood DisordersThese are a superordinate grouping of bipolar and depressive disorders. Mood disorders are defined according to particular types of mood and their pattern over time. Mood change is usually accompanied by a change in the overall level of activity; most of the other symptoms are either secondary to, or easily understood in the context of, the change in mood and activity. Thus, it is not surprising that the WHO-5 scores are amongst the lowest of the diseases reported.
Apart from the depressive episodes (reported above), mood disorders contains, amongst others, anxiety, and stress disorders. A total of 16 studies included patients with diagnosed stress and/or anxiety, mostly with the aim of testing support-training programs to improve the condition. The mean WHO-5 score at baseline was reported in 10 of them, with an average score of 36.3 ± 0.1. The largest study was performed in Japan, including 2295 participants, with the aim of examining the association between lifestyle behaviors and optimal well-being [27]. Authors found that participants without underlying diseases, who answered “always” (n = 411) to the question “Do you feel stressed?” had 35.9% lower well-being than those patients who answered “never” (n = 387): 67.8 ± 8.5 vs. 31.92 ± 8.0, respectively [27]. Bipolar disorders are characterized by two or more episodes in which the patient's mood and activity levels were significantly disturbed. Although the manuscripts do not specify the mood of the patients at the moment of scoring the WHO-5, the average of the seven papers (52.3 ± 0.9) reporting it was in line with other mental disorders.
Endocrine, Nutritional, and Metabolic DiseasesThe WHO-5 questionnaire was originally developed and validated in a study including patients with diabetes mellitus (DM) [11]. It is well known that living with DM can also produce psychological distress, and both patient and endocrinologist associations around the world recommend the use of psychological assessment with patient-reported outcomes (PROs) such as the WHO-5 [29, 30]. It is important to highlight that distress from DM is distinct from depression in that it is not a disorder but rather a psychological consequence of the disease [31].
Here, 107 of the 120 studies in this disease area reported the use of WHO-5 in patients with DM: 52 type 2 DM (T2DM), 25 type 1 DM (T1DM), and 30 including both types (Table 1; Table S3). The rest of the studies were focused on different thyroid-related diseases (n = 8), metabolic syndrome (n = 2), hypertensive nephropathy (n = 1), and irritable bowel syndrome (n = 1).
Diabetes MellitusMost of the studies on DM reporting the mean WHO-5 score (n = 89), described a similar mean ± SD to the European population 66.1 ± 0.3 and 60.3 ± 0.2 for T1DM and T2DM, respectively (Fig. 3; Table S3). These results indicate that people with a good control of the disease maintain good mental well-being. However, the heterogeneity amongst studies indicates that some patients, especially those with emotional distress, depression, or fear of hypoglycemia, have a low score [32,33,34,35,36,37]. In fact, in the 14 studies where the WHO-5 score was stratified, a range between 25 and 49% of the patients suffered from poor well-being (diabetes with distress; WHO-5 ≤ 50), with 11–21% of them showing moderate-to-severe depressive symptoms (WHO-5 score ≤ 28) [20,21,22].
Fig. 3
Representation of the main diseases reporting WHO-5 data. Dotted lines represent the mean of the general population (64.2), the threshold for depressive symptoms (WHO-5 = 50) and the threshold for major depressive symptoms (WHO-5 = 28), and blue area represents the standard deviation of the European countries weighted by number of inhabitants [91]. COPD chronic obstructive pulmonary disease, COVID-19 coronavirus disease 2019, IHD ischemic heart disease, IPF idiopathic pulmonary fibrosis, MS multiple sclerosis, RA rheumatoid arthritis, T1DM type 1 diabetes mellitus, T2DM type 2 diabetes mellitus, WHO-5 World Health Organization-Five Well-Being Index
In the same line, the two largest studies (one in Germany [38] and the other in 17 countries [39], included 17,563 T2DM adults, and 8596 T1DM/T2DM adults, respectively) identified worse glycemic control, insulin use, or severe hypoglycemia having a substantial negative impact on well-being. A lower level of well-being was also observed amongst women compared to men [38,39,40,41,42,43,44].
Diseases of the Circulatory SystemThe WHO-5 was used in 26 studies in the field of diseases of the circulatory system (Table S4), most of them including patients with ischemic heart diseases (IHD; n = 6) or with cerebrovascular diseases (n = 7).
Ischemic Heart DiseasesThe WHO-5 was reported in only four studies, all from the same research group in Denmark. The different studies screened patients with stable IHD and other comorbidities such as chronic stress syndrome (associated with increased sensitivity for pain), explaining the variability of the results, ranging from 53.1 ± 0.4 with high-pressure pain sensibility to 77.2 ± 0.6 in patients with low-pressure pain. Having metabolic syndrome or DM did not decrease the WHO-5 score in these studies.
Cerebrovascular DiseasesThis is a group of brain dysfunctions related to disease of the blood vessels supplying the brain, including strokes. Two studies measured the well-being of the patients either within the first 7 days from symptom onset [45] or at a minimum of 1 month after recovery [46], and interestingly both showed very similar WHO-5 scores (68.9 ± 22.9 and 68.0 ± 16.3, respectively), indicating normal well-being after recovery. However, another study only including patients who needed inpatient neuro-rehabilitation for more than 2 weeks, reported a higher impact on well-being, with an average score of 52.0 (range 4.0–76.0) [47].
Neoplasms (cancer)As mentioned above, absence of disease or disease remission are not necessarily related to being healthy or well-being; the oncology field is a clear example of this. According to the US National Cancer Institute, an individual is considered a cancer survivor from the time of diagnosis until the end of life, including those living with cancer and those free of cancer. This term is meant to capture a population of those with a history of cancer rather than to provide a label that may or may not resonate with individuals [48].
A study following a cohort of 4565 participants, 444 of whom were diagnosed with cancer, evaluated the well-being using the 8-item version of the Center for Epidemiologic Depression Scale, 0–2 years before a cancer diagnosis and 0–2 and 2–4 years post-diagnosis [49]. Besides an expected self-rated health deterioration following a diagnosis of cancer, the authors found that cancer survivors had poorer health and well-being than those without cancer, with no significant differences regarding the years post-diagnosis [49].
A total of 20 studies used the WHO-5 to evaluate the well-being of patients with cancer, 6 of them after diagnosis: 3 with breast cancer, 1 with lung cancer, 1 with head and neck cancer and the other study included participants with different cancers (Table S5). All 6 studies showed a similar score, with an average of 53.4 ± 0.5, indicating the emotional distress caused by a cancer diagnosis.
From the remaining 14 studies, the WHO-5 was evaluated and reported in 9 studies at least 1 year after follow-up in cancer survivors (3 breast cancer, 3 malignancies of women genital organs, and 3 studies with different types), with higher well-being levels: average WHO-5 = 60.0 ± 1.6. However, these results confirm that the well-being of cancer survivors might remain lower than the average population, even 1 or 2 years after disease remission.
Diseases of the Nervous SystemThis section includes diseases that affect the structure or function of the brain or spinal cord, which collectively form the central nervous system. Most the studies were evaluated in patients with epilepsy (n = 8) followed by multiple sclerosis and Parkinson disease with 2 studies in each condition (Table S6).
EpilepsyEpilepsy strongly impairs well-being, due to the burden of the disease and the uncertainty of the relapses. Here, in 4 of the 5 studies reporting WHO-5 in this population, the mean score was 32.6 ± 0.1. The uncertainty of the relapses might explain why these patients with an apparent absence of signs and symptoms (besides the relapsing period) maintain lower than expected WHO-5 scores. The last one, performed in Denmark, divided the patients dependent on co-existing psychological comorbidity (i.e., depression or anxiety). Those with psychological burden showed a similar score to those without (WHO-5: 36.6 ± 20.2); however, it is remarkable that those patients without other comorbidities showed a similar score to the general Danish population (72.6 ± 17.6).
Multiple SclerosisSuch patients are often pessimistic about their future [50]. However, the two studies reporting WHO-5 included patients with mild-to-moderate disability scores (based on the Expanded Disability Status Scale), which may explain the surprisingly high levels of well-being. One study from the United States showed an average score of 56.4 ± 9.8 [51], while the other study from Denmark correlates well-being with fatigue, showing the lowest score in those patients experiencing secondary fatigue (WHO-5 score = 58) and the highest in those not experiencing fatigue (WHO-5 = 80) [52].
Parkinson DiseaseThis is another disabling and progressive disease that affects the motor system. Two studies reporting WHO-5 (from the same research group) found average scores of 44.2 ± 20.0 and 51.7 ± 19.3. The impact of well-being is remarkable, considering that patients included in both studies are classified as having mild-to-moderate disability (severity score from 1 to 3 in the Hoehn and Yahr scale).
Diseases of the Musculoskeletal System or Connective TissueThis group comprises diseases of the muscles, joints and bones including autoimmune and non-autoimmune disorders. The overall mean WHO-5 of the 15 studies included here was 56.5 ± 0.2, indicating impaired well-being compared to the general population (table S7).
The studies included patients with arthropathies [rheumatoid arthritis (RA), n = 5 or osteoarthritis (n = 2)] or with conditions associated with the spine [scoliosis (n = 4) and axial spondyloarthritis (AxSpA, n = 3)].
The largest study performed in patients with inflammatory rheumatic diseases, included 4711 RA patients reporting WHO-5, with an average score of 57 ± 25 [53]. The score strongly correlated with the severity of the disease (r = 0.79). Unfortunately, the raw scores were not shown. The same study also included 782 patients with AxSpA, with a similar WHO-5 score (53.0 ± 23.0). Finally, 3 studies in the same cohort of patients reported a WHO-5 of 54.0 ± 11.5, similar to other diseases of this group (Table S7).
Diseases of the Genitourinary SystemThe genitourinary system includes the organs of the reproductive and urinary systems. These are grouped together because of their proximity to each other, their common embryological origin, and the use of common pathways. However, diseases in this category are quite diverse. Here, 11 studies used the WHO-5 for diseases of the reproductive system (n = 7) and urinary system (n = 4) (Table S8). In addition, 5 other studies evaluated the psychological burden of patients with infertility. Although infertility does not cause any physical impairment, it is well known that couples who cannot have children might feel incomplete and this could potentially impact their psychological well-being [54]. In fact, this is reflected by the low WHO-5 scores (38.9 ± 0.1) below the threshold of emotional distress, with similar impact between women and men [55,56,57].
Diseases of the Respiratory System (excluding COVID-19)Living with a lung condition is more likely to be associated with poor mental well-being due to the difficulty in performing daily activities or the fear of being unable to breathe [58].
AsthmaAsthma is characterized by variable and recurring episodes of wheezing, coughing, chest tightness, and shortness of breath [59]. Neither of the two studies on asthma reported the mean WHO-5 score (table S9). However, it is interesting to note that one study including patients with moderate-to-severe asthma, stable on inhaled corticosteroids, and case controls found a significantly higher proportion of asthmatic patients with psychological distress (WHO5 < 50: 68.6%) compared to controls (22.5%; OR = 7.5; 95% CI 4.02–14.04) [60]. The other study, a worldwide survey in severe asthma, reported the average per each of the 5 questions, showing a high impairment of well-being [61].
Idiopathic Pulmonary Fibrosis (IPF)This is a fatal disease that usually affects adults between the ages of 50–70 and is characterized by progressive decline in lung function resulting from fibrosis. Three studies from the same research group reported some distress, with a mean WHO-5 score of 56.2 ± 0.1 (table S9). In these studies, a high proportion of patients were stable, with mild or moderate IPF. However, the levels of impairment in these patients were notable.
Chronic Obstructive Pulmonary Disease (COPD)This is a type of progressive lung disease characterized by long-term respiratory symptoms and airflow limitation [62]. COPD impacts everyday activities such as walking or dressing, and, although incurable, can be treated symptomatically. A study including 158 COPD patients (149 of them reporting severity: 18 mild, 78 moderate, 39 severe, and 14 very severe), reported a WHO-5 mean score of 53.4 ± 24.0, similar to IPF patients and significantly lower than the general population [63].
Diseases of the SkinThe skin is the only organ which is completely visible, and patients with dermatoses are frequently stigmatized due to revulsion or fear of contagion [64]. Thus, it is not surprising that about 25% of people with skin disease also show depression, anxiety, or somatoform reactions, including 4–10% of patients with suicidal thoughts [65]. However, the use of WHO-5 to evaluate the well-being of patients with skin conditions is still poor. Four studies in patients with psoriasis included two in women with lichen sclerosus, and another study included patients with various skin conditions (table S10).
The International Alliance of Dermatology Patient Organizations (also known as GlobalSkin) has recently launched the Global Research on the Impact of Dermatological Diseases project aiming to collect global data on the impact of dermatological conditions on patients’ lives [66]. They have collected responses, including the WHO-5 questionnaire, from 4118 individuals spanning 96 countries and across 102 skin disease areas; however, the results are not yet available.
PsoriasisPsoriasis is a common, chronic, relapsing, inflammatory skin disorder characterized by abnormal epidermal keratinization and hyperproliferation. The first dermatological study to use the WHO-5 was in patients with moderate to severe psoriasis in 2017 [67]. Despite the severity of psoriasis, patients were treated with conventional rather than biologic therapies: topicals and/or methotrexate, acitretin, or ciclosporin; the overall WHO-5 score was 53.8 ± 27.0. A second study from China found significant differences in well-being depending on the severity of the disease: 58.2 ± 10.7 in patients with mild [Psoriasis Area and Severity Index (PASI) < 7)] versus 47.8 ± 12.0 in severe disease (PASI > 12) [68]. A larger study performed in Germany, used the WHO-5 for the first time under routine conditions in adult patients with psoriasis (baseline and 12 weeks follow-up) [69]. The study included patients with a good control of psoriasis (mean PASI = 2.4 ± 4.2) and therefore minimal disease, which might explain why the WHO-5 scores are close to the general population for both time points: 62.4 ± 11.2 and 65.6 ± 10.8, respectively.
A recent study conducted in Italy reported on the improvement in well-being among patients with moderate-to-severe psoriasis treated with two different doses (100 mg and 200 mg) of the biologic tildrakizumab, an IL-23p19 inhibitor. At baseline, patients exhibited significant well-being impairment, with scores of 17.5 and 18.0 for the 100 mg and 200 mg doses, respectively. However, after 28 weeks of treatment, all patients reported well-being scores exceeding the average score of the Italian population (59.6): specifically, 73.9 ± 6.3 for the 100 mg dose and 88 ± 5.0 for the 200 mg dose.
Diseases of the Optical SystemIs it not surprising that data from the 2004 Survey of Health, Ageing and Retirement in Europe, which included more than 22,000 older people, found that people with poor vision have a higher probability of losing interest and enjoyment in their activities; feeling fatigued, irritable, sad, and tearful; having less hope for the future; and wishing for death [70]. The only two studies using the WHO-5 have shown moderate impairment on well-being, with mean scores of 55.4 ± 26.3 and 58.8 ± 10.8, respectively [71,72,73]. However, the high dispersion of the results (SD) indicated that patients reported different levels of impaired well-being (Table S11). Although patients were not stratified, the authors explain that well-being depends on the adaptation to the vision loss, mental or physical health, the social support perceived, the strength of the spiritual/religious beliefs, and the personality traits and coping strategies used [71,72,73].
Coronavirus Disease (COVID)-19Although the COVID-19 crisis was, in the first instance, a physical health crisis in the first year of the pandemic, the global prevalence of anxiety and depression increased by a remarkable 25% [74]. Thus, it is not surprising t
Comments (0)