
Remember me



Exogenous insulin aims to replicate the natural insulin profile of individuals with normal glucose tolerance, closely mimicking the body’s physiological insulin response.
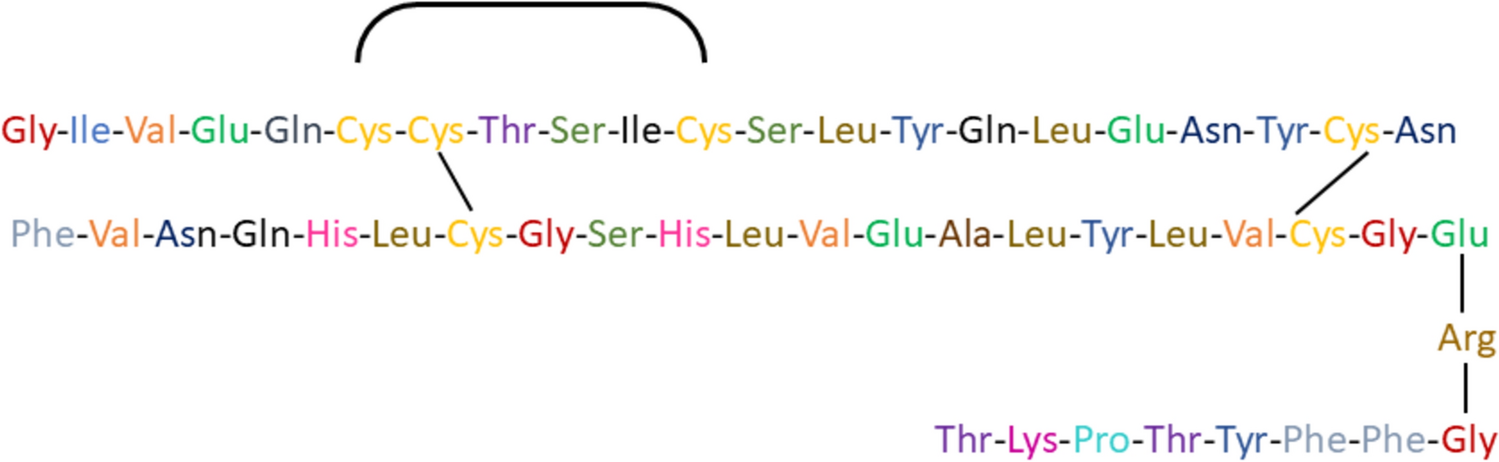
Biologically active insulin exists as a monomer composed of two polypeptide chains: the A chain (21 amino acids) and the B chain (30 amino acids), linked by two disulfide bridges (A7–B7 and A20–B19), with an additional intrachain disulfide bond in chain A (A6–A11) (Fig. 1) [10] Structurally, insulin is stored as hexamers in pancreatic β-cells, where zinc-mediated aggregation leads to dimer formation and further assembly into a stable quaternary structure. The hydrophobic core of the monomer enhances insulin stability, while its nonpolar surfaces facilitate dimer and hexamer formation, required for insulin storage and regulated release. Upon exogenous insulin administration, the hexamers dissociate into monomers for rapid physiological action [11].
Fig. 1
Molecular structure of insulin
In clinical practice, three main types of pharmaceutically produced insulin preparations are available [12]:
(1) Animal Insulins (Mid-1920s)These insulins were historically extracted and refined from bovine or porcine sources. However, their usage has significantly declined, with only a small fraction of patients currently relying on them. It has slower onset of action and increased risk of developing antibodies. While animal insulins are not sold in most regions, some limited contexts or specific geographical areas may still allow for their use. See Table 1 [13].
Table 1 Examples of animal, human, and analog insulin2. Human Insulin (1970s)This type of insulin is genetically engineered to have an amino acid sequence identical to that of endogenous human insulin. The advent of human insulin marked a significant milestone in diabetes management, offering an effective and well-tolerated treatment option for a broad spectrum of patients. See Table 1 [14].
3. Insulin Analogs (Late 1990s)Engineered through genetic modification, insulin analogs closely mimic human insulin, albeit with slight alterations in their amino acid sequence. This modification allows for the fine-tuning of insulin properties, such as onset, peak action, and duration, thereby enabling a more tailored and personalized approach to diabetes treatment. Insulin analogs are also superior to human insulin in terms of lowering the occurrence of hypoglycemia. See Table 1 [15].
As animal insulins have largely fallen out of favor, the focus has shifted towards the widespread utilization of human insulin and insulin analogs, which offer improved therapeutic precision and efficacy in the management of diabetes.
Furthermore, a biosimilar is a replica of an already authorized biological medicinal product, demonstrating similarity in physicochemical characteristics, efficacy, and safety through a comprehensive comparability exercise. Due to their complex size, structure, and manufacturing processes, biosimilars differ from simple generics. Policymakers and governments advocate for the growing biosimilars market, driven by their lower cost compared to innovator products. Some biosimilars are approved by the US FDA (Food and Drug Administration) as interchangeable biosimilar products, allowing substitution without prescriber intervention, commonly referred to as “pharmacy-level substitution,” like generic drug practices. Biosimilars and interchangeable biosimilar products have the potential to reduce healthcare costs, akin to generic drugs, by demonstrating high levels of structural (Table 2), biological activity, efficacy, safety, and immunogenicity profile similarity [16, 17]. In this review, we have also provided a comprehensive list of the trade names and manufacturers of currently available biosimilars and innovators on the market.
Table 2 Molecular differences among animal insulin, human insulin, and human insulin analogsInsulins can be classified based on their onset and duration of action, providing clinicians with a diverse array of options to accommodate the specific needs and requirements of individuals with diabetes (Table 3).
Table 3 Comparison of different types of insulin: onset, peak, duration, and timing of administration1. Long-Acting Insulins and Basal InsulinsThese insulins are designed to suppress hepatic gluconeogenesis, preventing the elevation of glucose levels during the fasting state, particularly in individuals with compromised endogenous insulin secretion. Moreover, their unique molecular modifications enable them to deliver relatively flat and protracted basal insulin levels [18].
Insulin GlargineInsulin Glargine (U-100) is characterized by its unique mechanism. Upon injection, it precipitates into stable hexamers within a physiologically pH-neutral environment, thereby extending its dissociation and subsequent absorption. This insulin can be administered once daily at any time of the day or, in cases of higher doses (typically exceeding 50 units daily), it may be given twice daily to effectively maintain its relatively consistent action profile [19].
Insulin DetemirThe structural modification in insulin detemir contributes to a delayed absorption process by promoting increased self-association at the injection site (hexamer stabilization) and facilitating strong, reversible binding to albumin within the subcutaneous tissue. Moreover, the interplay between insulin detemir and albumin in the bloodstream post-absorption aids in maintaining a more consistent time-action profile, serving as a safeguard against sudden fluctuations in the plasma concentration [20].
With the availability of more advanced options, manufacturers are no longer actively promoting detemir as they once did.
2. Ultra-Long-Acting InsulinsThese are insulins designed to initiate action within 30–90 min and maintain their effectiveness for over 24 h.
Insulin DegludecInsulin degludec represents a modified ultra-long-acting analog insulin. It forms multi-hexamers post-subcutaneous injection, leading to a gradual release of insulin monomers into the circulation, thereby extending its action duration. With a half-life of approximately 25 h and a duration of action exceeding 42 h, degludec exhibits stable insulin levels within 3 days of initial administration, resulting in reduced variability throughout the day compared to glargine insulin. The shelf life of insulin degludec is typically 2–3 years when stored unopened in a refrigerator (2–8 °C or 36–46 °F). Once opened or in use, insulin degludec can be stored at room temperature (< 30 °C or 86 °F) for up to 56 days (8 weeks). After this period, any remaining insulin should be discarded, as its effectiveness may be reduced [21].
Insulin Glargine U-300Gla-300 exhibits flatter pharmacokinetics and pharmacodynamics compared to Gla-100, leading to a more even distribution over 30–36 h at clinical doses for individuals with 68 + diabetes. This characteristic helps reduce the risk of overall and nocturnal hypoglycemia, including severe episodes, while achieving similar improvements in glycemic control. This distinction contributes to diminished intraday variability and enhanced day-to-day consistency. The shelf life of insulin glargine U-300 (Toujeo) is typically 2–3 years when unopened and stored in a refrigerator (2–8 °C or 36–46 °F). Once in use or opened, insulin glargine U-300 can be stored at room temperature (< 30 °C or 86 °F) for up to 42 days (6 weeks). After this period, any remaining insulin should be discarded to ensure potency and effectiveness [22, 23].
Insulin IcodecInsulin icodec is a novel basal insulin analog designed for once-weekly administration in individuals with diabetes. This analog insulin includes three amino acid substitutions and a C20 icosane fatty diacid chain, which allows it to bind reversibly to albumin, similar to insulin detemir. These modifications extend icodec’s half-life to approximately 196 h (around 7 days). One unit of icodec provides the same glucose-lowering effect as 1 unit of daily basal insulins, making the equivalent once-weekly dose seven times that of a daily basal insulin [24].
Initiation of Insulin IcodecBased on current studies, insulin icodec can be initiated with a weekly dose of 70 units, which is comparable to starting with 10 units per day of a once-daily basal insulin. It typically takes 3–4 weeks to reach a steady state. For those already using daily basal insulins like degludec, detemir, glargine U100, or NPH, the initial icodec dose can be calculated from their total weekly dose of their current insulin. However, studies have shown that a 50% loading dose can be beneficial when initiating icodec. The first dose of icodec can be administered at any time of the day, regardless of when the last dose of the previous insulin was taken.
Dose Adjustment and Titration
For dose titration, adjustments are typically made weekly. If fasting blood glucose levels are above the target range, the dose may be increased by 20 units. Conversely, if fasting blood glucose levels are below the target range, a similar 20-unit decrease can be made. To guide these adjustments, it is recommended that patients measure their fasting blood glucose on 2 days before and on the day of their weekly dose [25].
Onset of action: 1–2 h
Peak of action: Minimal peak
Duration of action: Up to 7 days
Timing of administration: Once weekly
Trade name: Awiqli (Novo Nordisk) (Innovator) (2024, launched in the Canadian market). As of November 4, 2024, insulin icodec had not received approval from the US Food and Drug Administration (FDA) [26].
3. Short-acting Insulins or Regular InsulinsRegular insulin is commonly administered prior to meals to mitigate the sharp increase in post-meal glucose levels. Upon subcutaneous injection, regular insulin undergoes the formation of hexamers, thereby decelerating its absorption rate. These hexameric structures gradually disassemble into insulin dimers and monomers, which are readily absorbed. Consequently, regular insulin exhibits a delayed onset of action, typically ranging from 30 to 60 min. To effectively counteract the surge in blood glucose after meals, it is recommended that regular insulin be administered approximately 30 min before meal consumption [14, 27].
4. Rapid-acting InsulinsRapid-acting insulin analogs are a result of modifications to the amino acid structure of human insulin, inducing reduced formation of hexameric insulin post-subcutaneous injection. This alteration facilitates faster insulin dissolution into monomers, hastened insulin absorption into the bloodstream, and a shorter period of activity. Although the in vivo potency matches that of regular human insulin on a molar basis, it elicits higher peak concentrations. Consequently, transitioning from regular to a rapid-acting insulin analog may necessitate a reduction in the insulin dosage. Compared to regular insulin, rapid-acting insulin analogs yield lower postprandial hyperglycemia and reduced incidences of late postprandial hypoglycemia. Optimal reduction of postprandial glucose excursions is achieved when administering rapid-acting insulin analogs 15–20 min before meals [27, 28].
Insulin LisproInsulin lispro was the first short-acting, genetically engineered insulin analog to be used in clinical practice. It is created by substituting proline at B28 with lysine and lysine at B29 with proline in the B chain of the insulin molecule. In solution, insulin lispro exists as hexamers but dissociates rapidly into monomers upon subcutaneous injection, leading to quicker absorption from the injection site. This rapid dissociation results in faster plasma insulin peaks and a quicker return to pre-injection levels compared to regular human insulin (RHI). The approval of insulin lispro for injection both before and right after a meal has proven beneficial, especially for parents of young children with type 1 diabetes and for hospitalized patients requiring insulin, particularly when the quantity of carbohydrates consumed during a meal remains unpredictable [29,30,31].
Insulin AspartInsulin aspart closely resembles regular human insulin (RHI) and endogenous insulin, with the exception of a single modification: proline at position 28 in the C-terminal region of the insulin B chain is replaced with an aspartic acid residue. Similar to lispro, insulin aspart exists as hexamers in solution but rapidly dissociates into monomers upon subcutaneous injection. This dissociation accelerates its absorption, allowing for a faster onset of action. The aspartic acid substitution does not alter the receptor-binding region of the insulin molecule, so the biological activity of insulin aspart remains unaffected in vivo [31,32,33].
Insulin GlulisineGlulisine is a fast-acting insulin analog with a rapid onset and shorter duration of action, approved by the FDA in 2004 for use in adults with T1DM and T2DM. It is distinguished from regular human insulin by two amino acid changes on the B chain: asparagine is replaced with lysine at position B3, and lysine is replaced with glutamic acid at position B29. Unlike lispro and aspart, insulin glulisine exists primarily as monomers in solution, which eliminates the need for dissociation and enhances its absorption rate. These characteristics contribute to its rapid onset of action [31, 34, 35].
5. Ultra-rapid-acting InsulinsUltra-rapid-acting insulin analogs have undergone enhancements by incorporating an excipient that interferes with the formation of insulin hexamers, thus accelerating their disintegration into dimers and monomers.
Fast-acting AspartFaster aspart has been modified through the inclusion of two excipients, namely l-arginine, to guarantee formulation stability, and niacinamide, which promotes improved absorption following subcutaneous administration [36].
Ultra-rapid-acting LisproUltra-rapid lispro is engineered with treprostinil and citrate to augment the absorption of insulin lispro [37, 38].
6. Intermediate-acting InsulinNPH (Neutral Protamine Hagedorn) insulin is an isophane suspension of human insulin and is recognized as an intermediate-acting insulin, emulating the physiological action of basal insulin. NPH insulin provides a steady and prolonged release of insulin. Additionally, it has demonstrated efficacy in managing gestational diabetes [39].
Premix InsulinPremix insulin represent a consolidated blend of rapid or short-acting insulins and intermediate- or long-acting insulins designed to address both fasting and postprandial glycemic control. The versatility of premix insulin allows for once, twice, or thrice daily dosing, adapting to the specific needs of individuals with diabetes. However, one con of premix insulin is that it lacks flexibility of dosing, as the fixed ratio of components may not allow for precise adjustments to meet varying daily glucose levels or carbohydrate intake.
These formulations are strategically crafted to optimize pharmacokinetics, ensuring a balance between 24-h efficacy and patient convenience. This nuanced design contributes to the notable adherence rates observed with premix insulin, fostering improved glycemic control. The combination of therapeutic effectiveness and user-friendly dosing regimens makes premix insulin a favorable choice in diabetes management [40].
The conventional biphasic human insulin in premix formulations comprise regular human insulin and NPH in ratios of 30/70 or 50/50. Administered approximately 30 min before meals, these formulations exhibit an action duration lasting between 10 to 16 h [41].
Onset of action: 0.5 h
Peak of action: 2–8 h
Duration of action: 14–24 h
Timing of administration: generally, two or three times a day before mealtime
Trade names: Humulin 70/30 (Eli Lilly) (innovator): 70% NPH insulin and 30% regular insulin
Insuman Comb 25 (Sanofi) (Innovator): 25% short-acting 75% isophane insulin
Huminsulin 30/70 (Eli Lilly): 70% isophane insulin and 30% short-acting insulin (used in specific markets under the Eli Lilly umbrella with slight formulation differences due to regional regulatory or manufacturing considerations)
Huminsulin 50/50: 50% isophane insulin and 50% short-acting insulin
Biosimilars: Novolin 70/30/ Mixtard 30/70 (Novo Nordisk), Actraphane 30/70 (Novo Nordisk), Wosulin 70/30 (Wockhardt), Gansulin 70/30 (Biocon), Insugen 30/70 (Biocon), Insugen 50/50, Rekool 70/30 (Torrent), ReliOn 70/30 (Walmart brand), Recomulin 30/70 (Reliance Life Sciences)
*The variability in insulin mixture ratios across regions is attributed to factors such as local regulations, healthcare standards, and market preferences, resulting in differences in available formulations.
In contrast, analog premix formulations present a faster onset of action, allowing administration up to 15 min prior to meals. Notably, compared to conventional premix counterparts, the analog formulations demonstrate prolonged activity, with durations ranging from 12 to 24 h [40, 41].
Onset of action: 0.1–0.3 h
Peak of action: 1–4 h
Duration of action: 16–24 h
Timing of administration: generally, two or three times a day before mealtime
Trade names: Novolog 70/30 (Novo Nordisk): 30:70- Aspart: Aspart Protamine, Humalog mix 75/25 (Eli Lilly): 25:75- Lispro: Lispro protamine, Humalog Mix 50/50 (Eli Lilly): 50:50- Lispro:Lispro protamine, NovoMix 50/50 (Novo Nordisk)
Comments (0)