Study sample
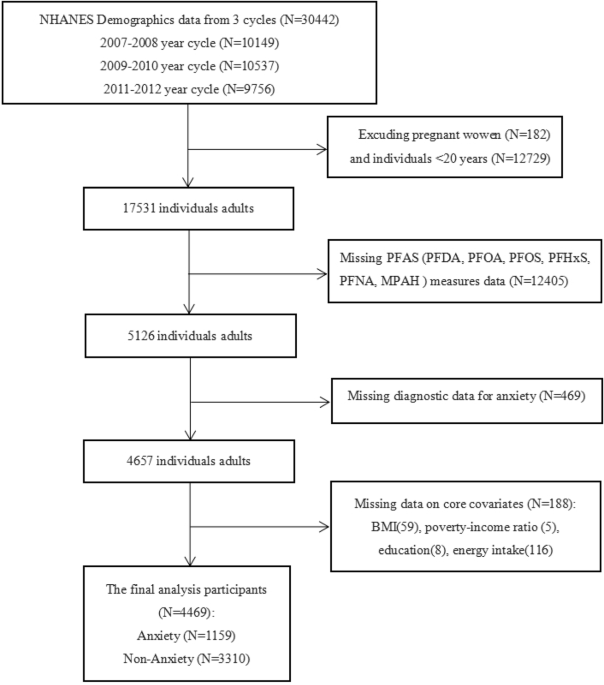
The current analysis uses data from pregnant participants in the Understanding Pregnancy Signals and Infant Development (UPSIDE) cohort study (Rochester, N.Y., USA) [40]. Between 2015 and 2019, the University of Rochester Medical Center and associated clinics recruited 326 pregnant participants based on the following criteria:(1) ≥18 years of age, (2) in the first trimester of pregnancy, (3) singleton pregnancy, (4) no major substance use issues or history of psychosis, (5) no major endocrine disorder (such as polycystic ovary syndrome), and (6) able to communicate in English. Study participants provided signed consent, and Institutional Review Boards at the University of Rochester and Rutgers University approved all study activities. Participants completed study visits in each trimester consisting of biospecimen collection and questionnaires on demographics, lifestyle, and health history. Placentas were collected at delivery. Of the 326 participants who enrolled in the UPSIDE study, 317 provided at least one urine specimen. Specifically, 301, 283, and 281 participants provided urine in the 1st, 2nd, and 3rd trimesters, respectively (Supplementary Fig. 1). One 1st trimester measurement that did not pass laboratory quality control standards was excluded, leaving 258 participants with mycoestrogen concentrations in all trimesters. Additionally, 274 placentas were collected at delivery, three were excluded from further study due to placenta abnormalities. The number of participants that contributed data to our primary analysis of urinary or placental predictors was 292.
Mycoestrogen concentrations
At three study visits across pregnancy (12.2 ± 1.3, 21.2 ± 1.8, 31.4 ± 1.9 weeks gestation) urine samples were collected. Specific gravity was measured using a refractometer (Atago 4410 PAL-10S Digital Hand-Held Pocket Urine Specific Gravity Refractometer, Tokyo, Japan), after which urine samples were frozen at −80 °C. Trained study coordinators collected placentas following standard protocols previously described [41]. Within 1 h of birth, study coordinators took samples of the fresh core villous tissue while leaving the maternal decidua surface intact. ~30 g of tissue was frozen in liquid nitrogen and stored at −80 °C. Detailed methods for placental processing have been previously described [42]. Urine and placenta samples were transferred on dry ice to the Environmental and Occupational Health Sciences Institute at Rutgers University for analysis.
Urinary (total; unconjugated plus conjugated) and placental (total) mycoestrogen concentrations (6 analytes: α-ZOL, β-ZOL, α-zearalanol (α-ZAL/ZER), β-zearalanol (β-ZAL), zearalanone (ZAN), and ZEN) were analyzed by ultra high-performance liquid chromatography-tandem mass spectrometry (UPLC-MS/MS) using previously published methods [42, 43]. In short, urine (0.4 ml) or placenta (~200 mg, homogenized) was combined with internal standards (D6-ZEN and D7- α-ZOL [Toronto Research Chemicals North York, Ontario, Canada]), sodium acetate buffer (pH 4.6 [Honeywell Fluka, Morris Plains, NJ, USA]), and deconjugation enzymes (β-glucuronidase, type HP-2, with sulfatase [Sigma-Aldrich #G7017, St. Louis, MO, USA]) for overnight incubation, in parallel with matrix matched calibration curves. Mycoestrogens were extracted with two sequential solid phase extraction steps (1st (urine): Chem ElutTM cartridges (1 ml, [Agilent Santa Clara, CA, USA], eluted with 3 × 2 ml methyl tert-butyl ether [MTBE]) or 1st (placenta): Chem ElutTM cartridges (3 ml, [Agilent Santa Clara, CA, USA], eluted with 3 × 5 ml MTBE; 2nd: Discovery DSC-NH2 cartridges [Sigma-Aldrich] with methanol) with intermittent drying under a nitrogen stream. Mycoestrogens were redissolved in HPLC solvent (for urine: 200 µl, for placenta 50 µl; 50% water, 25% acetonitrile, 25% methanol) and transferred to HPLC vials. Calibration curve samples were prepared from stock solutions (0.025–5.0 ng/ml) dissolved in acetonitrile (Sigma Aldrich ZEN: #Z2125, α-ZOL: #Z0166, β-ZOL: #Z2000, α-ZAL: #Z0292, ZAN: #Z0167, β-ZAL: #Z0417). Each run included blanks, quality control standards (analytes and the internal standard at 0.1 ng/ml in acetonitrile), and calibrator samples (0.025 ng/ml in matrix, duplicates). Concentrations were assessed by UPLC-MS/MS using a Dionex UltiMate 3000 UHPLC interfaced to a Thermo Scientific Q Exactive HF Hybrid Quadrupole-Orbitrap by Thermo Fisher Scientific (Waltham, MA, USA), run time parameters were previously published and details on quantitation are provided in the supplementary materials [42]. For analytes detected in >75% of samples, samples below the limit of detection were assigned a value of LOD/√(2) [44].
To standardize for urine dilution, we used the Boeniger formula: Pc = P[(SGmtri−1)/(SG−1)] where Pc is the specific gravity corrected analyte concentration, P is the mycoestrogen analyte concentration [45]. SGmtri is the trimester median specific gravity for the UPSIDE cohort, and SG is the individual’s urine specific gravity for the sample.
Estimating unconjugated and conjugated mycoestrogens
In phase 2 metabolism, mycoestrogens are conjugated by UDP-glucuronosyl transferases and sulfotransferases to produce glucuronide and sulfate conjugates presumably rendering them unable to interfere with ER α/β activity [3]. Therefore to understand endocrine disrupting potential of this exposure, we estimated the conjugated fraction in a subset of samples (n = 30, 10 per trimester). The subset was chosen because these participants had detectable levels of each analyte. Samples were prepared according to methods described above, except we omitted the enzymatic digestion step when measuring unconjugated mycoestrogens. Samples were prepared and quantified in parallel to assess percent unconjugated mycoestrogens relative to the total (unconjugated plus conjugated) concentrations.
Sociodemographic and perinatal predictors of mycoestrogen concentrations
Sociodemographic and perinatal variables were collected from questionnaires completed at prenatal visits. These included maternal age (categorized here as <25, 25–29, 30–34, ≥35 years), race/ethnicity (Non-Hispanic White, Non-Hispanic Black, Other race [Asian, Pacific Islander, Mixed Race, and Other], Hispanic), education (less than high school/high school, some college/bachelors, and any post-graduate education), parity (nulliparous/parous), use of social services during pregnancy (any vs. no use of Medicaid, the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC); or other public assistance), marital status (categorized here as married/living as married vs single/divorced/widowed/separated). We examined race/ethnicity as a proxy for structural racism which may affect access to resources including food [46]. Maternal height and weight at earliest prenatal appointment were used to calculate early pregnancy BMI (kg/m2) as a proxy for pre-pregnancy weight [47]. Because fungal growth on crops depends on weather and climate, mycoestrogen food contamination may follow seasonal patterns [37]. Season of biospecimen collection (urine or placenta) was categorized as spring (March, April, May), summer (June, July, August); fall (September, October, November), and winter (December, January, February). Finally, fetal sex differences in placental levels of environmental pollutants have been detected [48] and fetal-sex-specific impacts on health endpoints are often reported, therefore we considered fetal sex which was collected from the medical record.
Dietary predictors
As mycoestrogen exposure is considered to occur almost exclusively through contaminated foods in the general population (non-occupational exposure), we evaluated potential dietary predictors of exposure. A trained nutritionist with knowledge of regional foods, preparation techniques, and food in the marketplace, conducted 1–3 24-h dietary recalls per participant in mid-late pregnancy over the telephone. The United States Department of Agriculture (USDA)’s Automated Multiple Pass Method was used [49] to obtain diet consumed within prior 24 h. The recalls were then entered into the Nutrition Data System for Research software (NDSR, 2017 version, University of Minnesota Nutrition Coordinating Center, Minneapolis, MN) to derive nutrient intake [50]. Here we focus on participants with two recalls during the 2nd trimester (n = 172) [49]. For participants with two recalls, the second occurred 3–30 days after the first. Based on these recalls, we calculated (1) overall energy intake (kcal/day), (2) Healthy Eating Index (HEI), and (3) ultra-processed food (UPF) consumption, (4) percent of protein from animal sources, (5) percent of protein from vegetable sources.
Overall energy intake
The National Cancer Institute (NCI) has developed a statistical method to model aspects of usual dietary intake when the dietary assessment method is a Food Frequency Questionnaire (FFQ) or one to two 24-h dietary recalls [51]. This method was used to generate estimates of micro and macronutrient intake from food. In this analysis energy intake is estimated daily energy (kcals/day) from diet only.
The healthy eating index (HEI)
The HEI is a measure of diet quality used to assess how well a set of foods consumed aligns with key recommendations and dietary patterns published in the Dietary Guidelines for Americans (DGA) [52]. The HEI-2015 was used to score dietary recalls as the closest timing to our data collection (2015–2019). The maximum score is 100 and is derived from nine adequacy and four moderation food components; a higher score indicates closer adherence to the DGA and a healthier diet. The HEI-2015 adequacy components include [maximum points] total fruit [5], whole fruit [5], total vegetable [5], greens and beans [5], whole grains [10], dairy [10], total protein [5], seafood and plant protein [5], fatty acids [10] and the moderation components include refined grains [10], sodium [10], added sugar [10], and saturated fats [10]. The scoring standards for adequacy sub-scores are calculated based on volume of food group per 1000 kcal consumed. HEI-moderation sub-scores are calculated based on % of energy (added sugars or saturated fats) or volume/weight per 1000 kcal (refined grains, sodium). HEI total and sub-scores (adequacy and moderation) were calculated for each dietary recall. The HEI scores from two recalls from the second trimester were averaged.
Ultra-processed foods (UPF)
UPF are highly processed foods that contain ingredients intended to extend shelf life and make the food hyper palatable [53]. Our main measure of UPF was percent of calories in the diet deriving from UPF (UPF%). To calculate UPF%, first, unique food lists were compiled from participants’ dietary recalls and independently coded according the NOVA guidelines by two members of the research team [53]. The NOVA guidelines (not an acronym) are a system of classifying foods by the extent, nature, and purpose of food processing [53]. Differences in coding were resolved by a third rater. For composite foods (e.g., tacos, sandwiches), we disaggregated the components which were then individually coded. Based on those classifications, we determined the total calories coming from UPF. Finally, daily UPF% was calculated as (UPF calories/raw total calories)*100. The UPF% from two recalls from the second trimester was averaged.
Protein source
Given that prior literature links mycoestrogen exposure to meat consumption we examined protein source [5, 54]. Grams of total protein, animal protein, and vegetable protein were abstracted from NDSR output. Percentage of protein from animal or vegetable source was calculated for each participant dietary recall. Protein source variables were averaged from two dietary recalls for each participant.
Statistical analysis
Based on the prior literature, we created a composite measure of total mycoestrogen exposure (Σmycoestrogens) by summing analyte concentrations (i.e., ZEN, aZOL, bZOL, aZAL, bZAL, ZEN) from an individual’s sample [5]. We examined descriptive statistics (including percent above LOD, median, geometric mean, geometric standard deviation, and percentiles) for all analytes. Specific-gravity adjusted concentrations were log-transformed to improve normality. To examine reliability of mycoestrogen concentrations, we calculated intraclass correlation (ICC; two-way, consistency) across time periods (1st/2nd, 2nd/3rd, 1st/3rd, 1st, 2nd, 3rd). We used chi-square tests to examine independence of the categorical predictor variables.
In our primary analysis, we fitted linear mixed effect models with log-transformed urinary concentrations as the response variable and sociodemographic and perinatal factors as predictors (fixed effects). We considered three outcomes (concentrations of aZOL, ZEN, and Σmycoestrogens) as the rest of the analytes were detectable in only a small fraction of samples. We first created individual models for each predictor including a random effect for each participant. Additionally, we examined mutually adjusted models that included all predictors that were significant in unadjusted models (urine or placenta models) at p < 0.05. All of the following covariates are included in the mutually adjusted models for urine were: maternal age, BMI, ethnicity/race, education, parity, use of social services, marital status, fetal sex, season of urine collection, and sampling time (trimester: 1st, 2nd, 3rd). We additionally considered models with sampling time as a continuous variable (gestational weeks) and results were similar. In preliminary analysis, we additionally considered alcohol use and smoking in pregnancy, but they were dropped from further consideration due to lack of association with any concentrations. Due to the high variability of concentrations across pregnancy, our primary analysis consisted of participants who contributed urine samples in all trimesters; secondarily we analyzed predictors amongst participants who had at least one urine sample (n = 317).
We additionally considered predictors of placental mycoestrogens using generalized linear models or logistic regression models. ZEN (as a dichotomous variable (detect/non-detect) and Σmycoestrogens (continuous) were the response variables in these models, because individual placental metabolites were detected in <75% of samples. In the placental models where the response variables were log-transformed Σmycoestrogens concentrations, we used generalize linear models. We additionally used logistic regression models with ZEN as a binary variable (non-detect/detect). Predictors were first considered individually in unadjusted models. Subsequently, we fitted mutually adjusted models including maternal age, BMI, ethnicity/race, education, parity, use of social services, marital status, fetal sex, and season of placenta collection. Covariates were included if they were associated with mycoestrogen concentrations (urinary or placental) at p < 0.05. We examined independence of covariates with chi-square test.
For both urine and placental predictors, for ease of interpretation, we calculated a ratio (concentration compared to reference group) by exponentiating the beta estimate, and confidence intervals limits. Ratios <1.0 and >1.0 indicate lower or higher exposure than the reference group, respectively [55, 56]. We additionally report ß estimates and 95% confidence intervals in supplementary material. We performed multiple sensitivity analysis. First, we examined predictors of aZOL concentrations in participants who had detectable aZOL (n = 252 participants, n = 649 measurements), to eliminate any potential bias caused by replacing missing values with LOD√2. Second, we performed a sensitivity analysis including three placentas that were partially delivered and which were excluded from the primary analysis.
In the analysis of dietary predictors, we examined associations between dietary factors (total daily energy intake, HEI total, HEI sub-scores [total fruit, whole fruit, total vegetable, greens and beans, whole grains, dairy, total protein, seafood and plant protein, fatty acids, refined grains, sodium, added sugar, saturated fats], UPF%, % of protein from animal sources, % of protein from vegetable sources) and 2nd trimester mycoestrogen concentrations to match timing of exposure measurement with duplicate dietary recalls. We examined Pearson correlations between all dietary parameters considered. Dietary factors as predictors were considered individually in unadjusted linear models. In adjusted models, we include covariates identified in predictors analysis (maternal age, race/ethnicity, parity, education, season of urine collection, marital status, use of social services). For ease of interpretation of regression results, HEI-moderation sub-scores estimates (sodium, added sugars, refined grains, saturated fats) were multiplied by −1 so that higher score indicated higher consumption of that dietary component. In a sensitivity analysis of dietary predictors, to account for correlation of HEI subscores, we considered models where we additionally adjusted for total HEI score minus the subscore predictor [57, 58]. In a post hoc analysis, we examined differences in diet quality by levels of sociodemographic predictor of urinary mycoestrogen concentrations.
All analyses were performed in R Studio (Version 2023.06.1 + 524)


Comments (0)