In over fifty percent of initial magnetic resonance (MR) examinations conducted on newborns, frontal periventricular gray matter was observed in T2-weighted and diffusion-weighted imaging (DWI) modalities, frequently associated with frontal periventricular bands. These MR studies were performed for a range of clinical reasons, of which a third was not related to suspected hypoxic-ischemic injury. Typically, the imaging revealed that the frontal periventricular gray matter appeared symmetric. Furthermore, an inverse relationship was identified with gestational age, indicating that these developmental structures become less conspicuous as brain development progresses.
As MRI usage in preterm and term infants grows, an increase in the detection of subtle punctate lesions in white matter is observed [12]. Recent studies have linked the increased risk of white matter injury in preterm infants to the sensitivity of specific brain cells, like late oligodendrocytes. Research indicates infants with focal WM lesions show lower fractional anisotropy, suggesting widespread microstructural changes not visible on conventional MRI [13]. While WM injury is common in preterm infants, it is also seen in term newborns, particularly those with congenital heart disease and neonatal encephalopathy [9, 10, 14]. These findings highlight the significance of comprehending the diverse manifestations and underlying mechanisms of focal white matter lesions across various newborn populations.
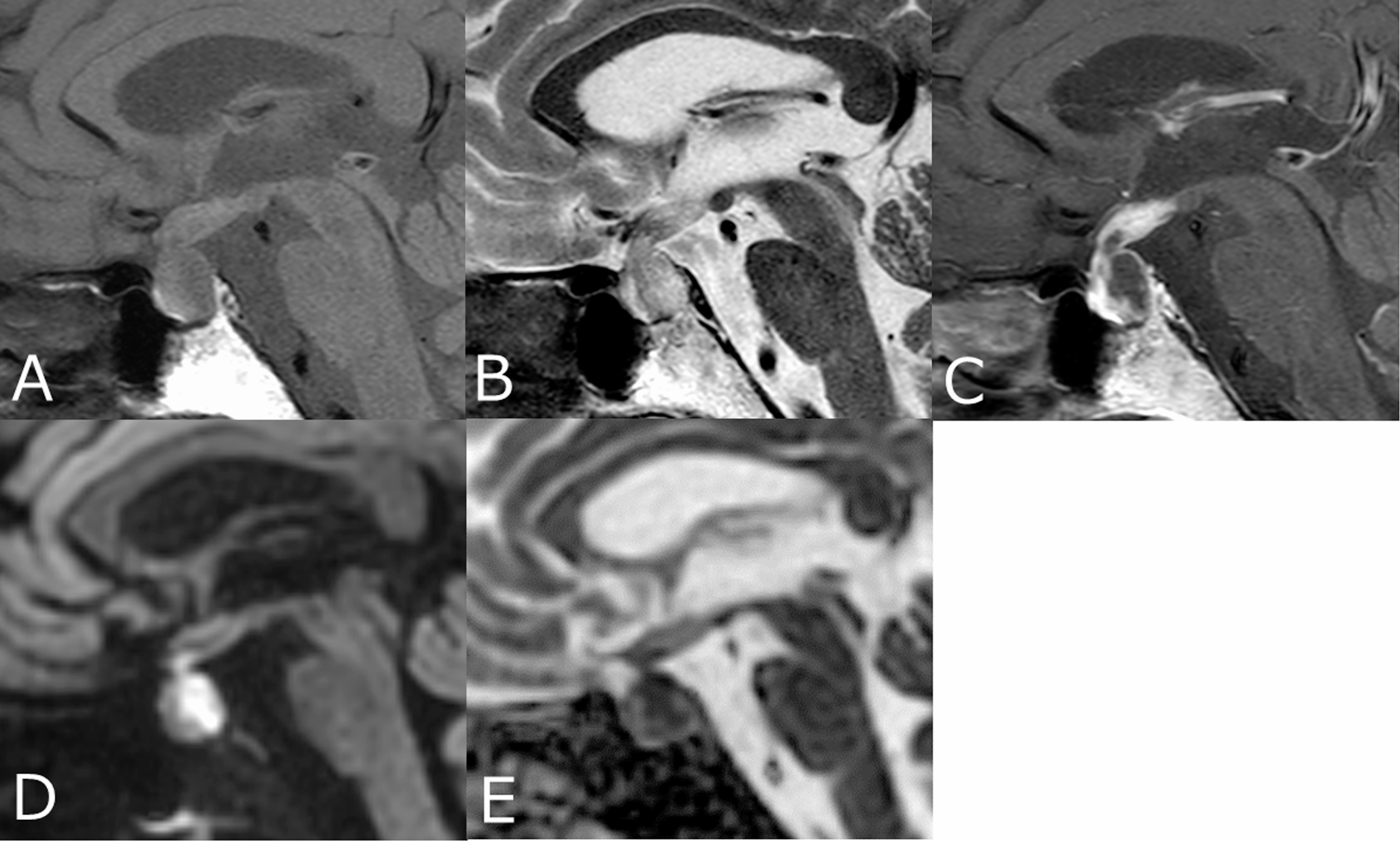
While hemorrhagic WM lesions can easily be identified on SWI, non-hemorrhagic WM lesions often show restricted diffusion (i.e., increased signal intensity on DWI with decreased ADC values), attributed to possible inflammatory or ischemic etiology. Restricted diffusion appears only on early scans, i.e., during the first week after injury [15]. In our study, apparently restricted diffusion of the frontal periventricular gray matter with lower ADC signal relative to adjacent non-myelinated WM can be misdiagnosed as focal WM injury, though ADC values are not low compared with adjacent opercular cortex. Furthermore, non-hemorrhagic WM lesions observed in early MRI scans commonly show a pronounced increased T1 signal, likely due to the onset of early gliosis [16, 17]. In our cohort, the similarity in the T1 signal of the frontal periventricular gray matter to the cortex or basal ganglia further makes the diagnosis of focal WM lesions unlikely. In our study, most patients' focal frontal periventricular gray matter appears symmetric, which is less characteristic of hypoxic-ischemic WM injury. The assessment of frontal periventricular regions in newborns using multiple MRI sequences is critical to distinguish between periventricular maturation remnants and focal white matter hypoxic-ischemic injury. The utilization of T2-weighted, DWI, ADC maps, and T1-weighted and SWI sequences provided valuable insights into the nature of these focal abnormalities.
Similar to periventricular bands, frontal periventricular gray matter is most probably developmental structures involuting brain maturation and represents residual fetal structures. Starting from the end of the second trimester of pregnancy, there is a significant diminution in the volume of the germinal matrix, consisting of densely packed neuronal and glial progenitors [1, 3, 4]. As gestation approaches term, the germinal matrix contracts to a minimal cellular layer adjacent to the ventricles. This final phase of involution of the germinal matrix is observed in near-term gestation overlying the caudate nucleus head as well in other sites as the apex of the temporal horns of the lateral ventricles and along the lateral wall of the occipital horn of the lateral ventricles. These relatively compact cells might result in a signal similar to the cortex, I.e., shorter T1 and T2 and reduced diffusivity, compared with surrounding non-myelinated WM. These embryological remnants are probably common in the early postnatal period, especially in preterms and young-term newborns. Our findings align with previously established data regarding the higher frequency of periventricular bands in younger premature infants scanned at term [5], extending these developmental imaging findings also to term newborns imaged shortly after birth.
Our study faced several limitations, including its retrospective design, leading to a heterogeneous cohort with MRI scans performed at various ages for different clinical reasons. This diversity and the absence of neurodevelopmental outcome assessments limited our ability to draw broader conclusions. However, we included newborns without clinical suspicion of hypoxic-ischemic injury and those who were evaluated for structural abnormalities detected in prenatal imaging with no clinical suspicion of hypoxic-ischemic injury as an “internal non-hypoxic-ischemic control group”. This internal control group enables highlighting the common findings of residual germinal matrix mimicking hypoxic-ischemic injury. Another limitation stems from the retrospective design of the study, which involved the use of different 3T scanners and varying sequence parameters. This introduced scanner-related variability in the detection of periventricular gray matter and periventricular bands.
To conclude, our study reveals that early MRIs of newborns frequently show frontal periventricular gray matter, often alongside frontal periventricular bands, suggesting developmental rather than hypoxic-ischemic origins. These findings, seen in preterm and term infants, highlight the complexity of diagnosing focal white matter (WM) injuries, emphasizing the need to carefully interpret MRI characteristics like diffusion and signal intensity.




Comments (0)