
Remember me



In our study we found that MRI findings of parenchymal involvement of primary and secondary CNS lymphomas were quite similar. However, tumor localization and proportion of edema in the VASARI feature set and infratentorial involvement and notch sign in other MRI features were significantly different between PCNSL and SCNSL.
We observed a predilection of PCNSL to predominantly involve the supratentorial compartment, especially frontal lobe (47.7%). Other studies reported frontal lob location in 20-49% of PCNSL patients, consistent with our results [7, 25]. Infratentorial involvement was present in 58.3% of patients with SCNSL and 15.8% of patients with PCNSL in our cohort. Previous studies have reported infratentorial involvement in SCNSL ranging from 16.7 to 42.9%, while in PCNSL, it has been reported between 34.6% and 50% [3,4,5, 26]. Compared to previous studies, infratentorial involvement of SCNSL was more common in our series. Among the SCNSL cases involving the infratentorial compartment, four had isolated infratentorial involvement, while three cases showed concomitant supratentorial involvement. Although infratentorial involvement is a more commonly expected finding in SCNSL, it can also be observed, though less frequently, in PCNSL.
To the best of our knowledge, the presence of the notch sign has not been reported previously in the differentiation of PCNSL from SCNSL. In our series, 73.7% of cases with PCNSL demonstrated the notch sign, whereas only one-third of cases with SCNSL showed this finding. The notch sign was defined as an abnormal deep indentation at the tumor margin on contrast-enhanced MR images of PCNSL patients [23]. In the study of Mansour et al., it was stated that the PCNSL occurs subcortically, respecting the adjacent cortex and its morphology, resulting in a crescent appearance [27]. We believe that the notch sign and crescent appearance represent the same radiological manifestations of equivalent morphological alterations. However, there are no studies examining either the notch sign or the crescent appearance in the SCNSL. While the notch sign serves as a valuable aid in differentiating between PCNSL and SCNSL, it is important to bear in mind that it may also be present in cases of SCNSL. We also observed that in cases with notch sign, this feature was exclusively caused by a tumor located in the supratentorial compartment. In our series, infratentorial involvement of SCNSL was more frequent than that of PCNSL. The cerebellum, which occupies a large portion of the infratentorial compartment, has a higher neuronal density and a more compact anatomical structure compared to the cerebrum [28, 29]. Since lymphoma is known as a plastic tumor, it can be hypothesized that the lower frequency of notch sign in SCNSLs is related to the compact structure of the cerebellum. However, this hypothesis needs to be investigated in larger case series.
Scoring of VASARI features which estimate proportion requires assesment of the entire MRI study. It is assumed that the entire signal abnormality consists of four different components: enhancing tumor, non-enhancing tumor, necrosis, and edema. We found that proportion of vasogenic edema was significantly higher in the PCNSL group. This finding, which seems to be helpful in differentiating PCNSL from SCNSL, has not been previously described. Compared to glioblastoma, PCNSL showed a higher degree of blood-brain barrier disruption within the tumor mass resulting in increased vascular permeability. Neoplastic lymphoid cells can easily expand the vascular wall by penetrating through the rich reticulin fiber network [30]. This blood-brain barrier disruption in the tumor mass is seen as increased vascular permeability and could correspond to vasogenic edema on MRI. In our study, the relatively higher occurence of multifocality/multicentricity and greater degree of perivenular contrast enhancement observed in cases of PCNSL compared to SCNSL may offer an explanation for the higher proportional prevalence of edema in this particular group. However, it is important to note that the higher peritumoral edema observed in the PCNSL group may not be generalizable due to the limited sample size and the history of prior steroid treatment in patients with SCNSL, where the shortest interval between imaging and steroid treatment was approximately three weeks in our cohort. These factors necessitate caution in interpreting the peritumoral edema difference and their applicability to broader patient populations. There is a also a need for dynamic contrast-enhanced MR studies evaluating vascular permability parameters such as Ktrans, Kep, and Ve to elucidate why the proportion of edema is higher in patients with PCNSL compared to SCNSL.
Hill et al. reported parenchymal involvement in only one third of cases with SCNSL in their review. However, in most of the articles reviewed in this article, the diagnosis was made by cerebrospinal fluid examination or CT findings or clinical data that were not radiologically correlated [31,32,33,34]. Parenchymal involvement may not have been detected in these studies since MRI evaluation was not performed. In contrary to these studies, parenchymal lesions were observed in all SCNSL cases in our series. 7/12 SCNSL cases had pial involvement and 9/12 had ependymal involvement. (Fig. 4). Similar to our study, Malikova et al. reported analyzing the MRI appearances of 21 patients with SCNSL, parenchymal involvement was reported in all but one patient [5]. Mass-forming parenchymal brain involvement has been reported as an uncommon form of invasion into the CNS for systemic lymphomas [35]. However, we found no significant difference in the type of parenchymal involvement (mass-forming versus pial/ependymal) between PCNSL and SCNSL.
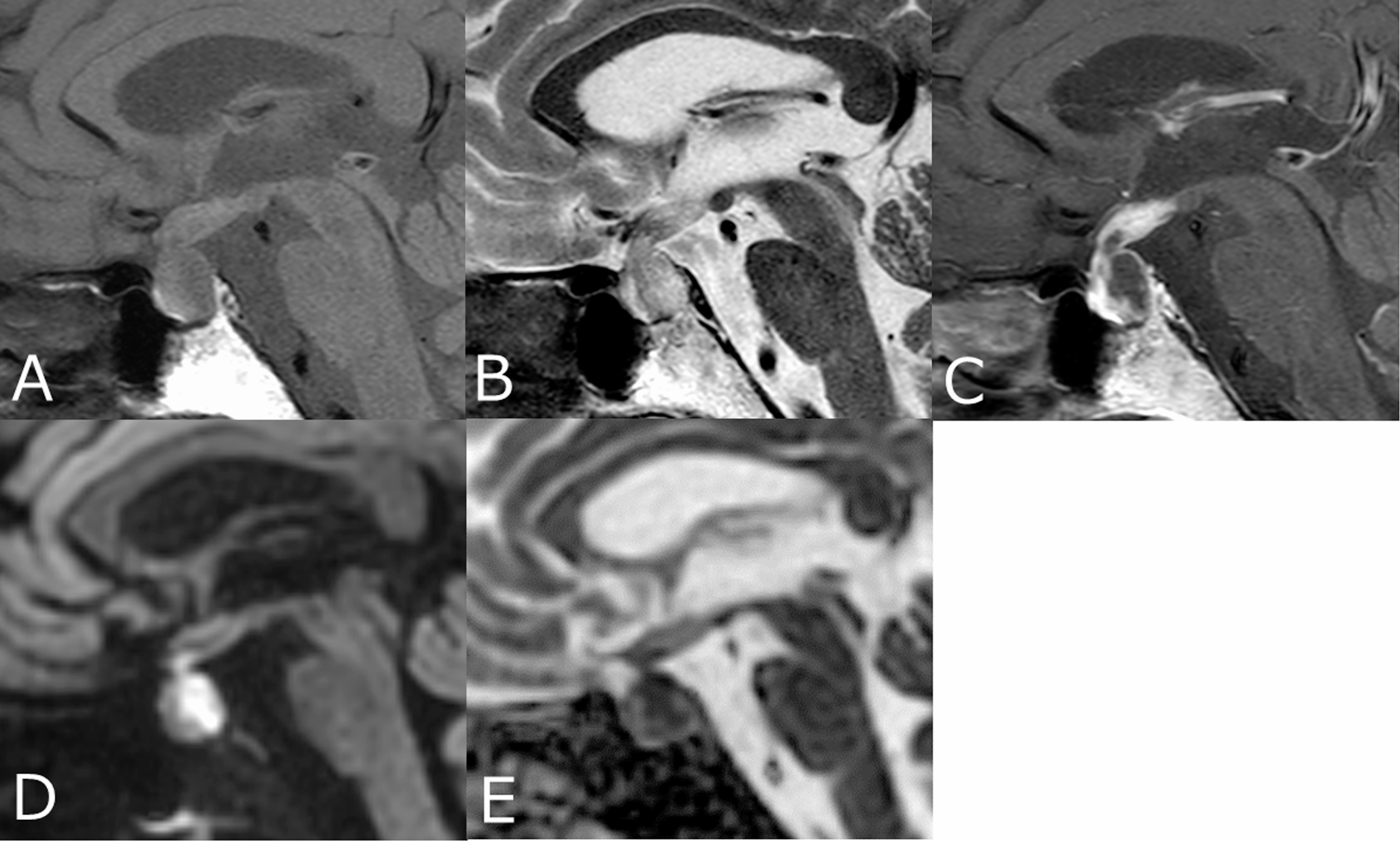
Fig. 4
An axial (a) C + T1W image of a 61-year-old male patient with SCNSL shows cerebellar leptomeningeal enhancement. The coronal C + T1W image (b) reveals a parenchymal lesion in the left frontal and temporal lobes, along with ependymal enhancement in the ipsilateral temporal horn (arrow)
In our study, almost perfect inter-reader agreement was observed in 9 out of the 25 VASARI features. Substantial agreement was achieved in 8 features, while moderate agreement was observed in 4 features. In the remaining four VASARI features, both readers made identical decisions. Both readers assessed contrast enhancement as marked and well-defined, while neither cyst nor calvarial remodelling was detected in any case. In a study evaluating the inter-reader agreement of VASARI features in pediatric brain tumors, acceptable agreement was found in 7 out of the first 25 features. Features with substantial agreement and almost perfect agreement were considered acceptable [36]. In a recent study by Setyawan et al.‘s, which utilized VASARI features for the prediction of grade and molecular parameters of gliomas, the inter-reader agreement was found to be between the kappa coefficent of 0.714 and 0.831 [37]. Given the high inter-reader agreement achieved in our study, we can assume that VASARI feature guide as well as other specific features can be used in the assessment of CNS lymphomas.
There are several limitations of the present study. The primary limitation of our study is the small sample size, which limits the broader relevance of our findings. Larger studies investigating the morphological MRI features of CNS lymphomas are needed to further validate our results. The variability in MRI protocols was due to the wide temporal scope encompassed by the retrospective study design. Therefore, diffusion-weighted images and susceptibility-weighted images were not obtained in some of the cases. Another limitation of the study is the visual assessment of the VASARI feature set rather than quantitative measurements. Additionally, the absence of immunocompromised cases in the evaluated PCNSL group hinders the generalizability of our results.
Comments (0)