
Remember me



This study was approved by the institutional review board of our hospital and conducted in accordance with the principles of the Declaration of Helsinki. The requirement for obtaining written informed consent was waived due to the retrospective nature of the study.
We studied 44 patients with MMD (63 hemispheres) who were previously revascularized with combined bypass surgery involving an STA-MCA single anastomosis with EMS, EDS, and/or encephalopericraniosynangiosis (23 hemispheres in 14 pediatric patients [age ≤ 15 years] and 40 hemispheres in 30 adult patients at surgery). After the bypass surgery, they underwent follow-up for postoperative bypass patency using TOF-MRA and silent MRA between January 2022 and December 2023. The mean duration from surgery to MRA was 8.5 years (range, 1.2–22.3 years). Table 1 shows the patient characteristics, including sex, mean age at operation, onset type, Suzuki stage, and mean follow-up period.
Table 1 Patient characteristicsDSA was performed approximately one year after surgery. In the period of this study, 13 patients (16 hemispheres) underwent postoperative DSA at the same session of both TOF-MRA and silent MRA (the mean duration from surgery: 14.1 months). We first reviewed direct and indirect bypass development of those patients in both types of MRA and the DSA images and subsequently rated the visualization of the neovascularized flow through the bypass in all 44 patients.
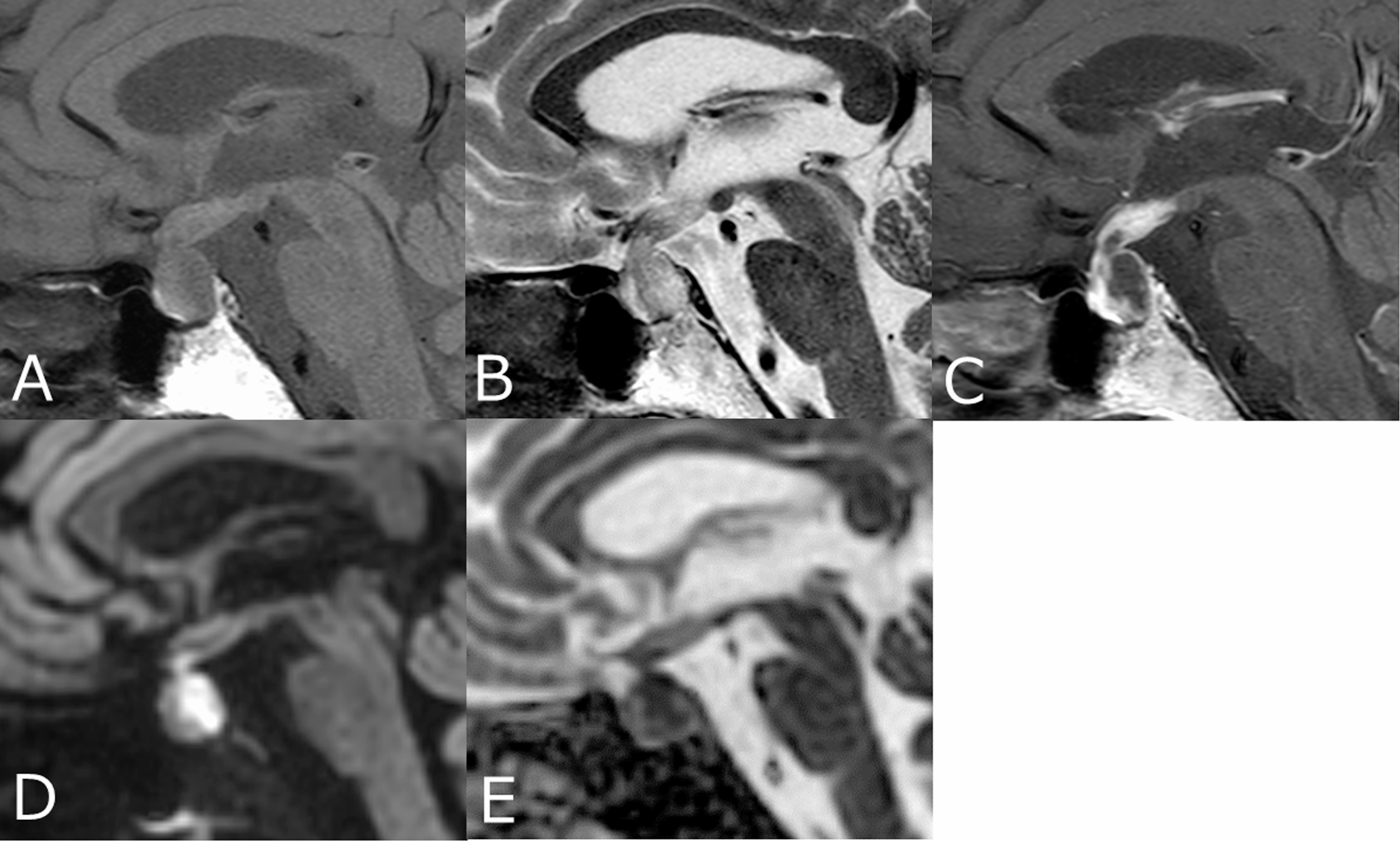
The exclusion criteria were as follows: (1) both types of MRA were not performed at the same session; (2) MRA and DSA have been performed more than one week apart; (3) poor image quality caused by motion artifacts. Two experienced neurosurgeons (one with 16 years and the other with 18 years of experience), independently reviewed the MRA and DSA images as a standard criterion and subjectively rated the visualization of the flow using a four-point scale as follows (Fig. 1): 0, not visible (near-complete or no patency of donor arteries); 1, poor (slightly visible donor arteries); 2, good (acceptable revascularization around the brain surface); and 3, excellent (good quality of revascularization with perfusion from the cortical surface into the MCA). We defined scores of 0 or 1 as poor bypass patency, 2 as good bypass patency, and 3 as excellent bypass patency.
Fig. 1
Grading score of postsurgical bypass patency on a four-point scale. (A) Grade 0, not visible (near-complete signal loss or no signal of donor arteries; white arrow); (B) grade 1, poor (slightly visible donor arteries; white arrows); (C) grade 2, good (acceptable revascularization around the brain surface; white dotted circle); (D) grade 3 in indirect bypass, excellent (good quality of revascularization with perfusion from the cortical surface into the middle cerebral artery; white dotted circle); and (E) grade 3 in direct bypass (white arrows)
Imaging techniques: silent MRA, TOF-MRA, and DSASilent MRA was completed in a single scanning session using a 3-T magnetic resonance imaging (MRI) scanner and a UTE sequence with combined arterial spin labeling (ASL). The UTE sequence minimizes phase dispersion, and ASL is used as a preparation pulse to visualize mild flow signal changes. Data acquisition is based on a 3D radial scan, and control images are acquired before pulse labeling. The control and labeled images are subtracted to yield an angiographic image, thereby improving the multidirectional slow blood flow visualization on the cortical surface.
In our hospital, the scan parameters of silent MRA (Discovery MR 750 w 3.0T; GE Healthcare, Chicago, IL) were as follows: repetition time (TR), 791 ms; echo time (TE), 0.020 ms; flip angle, 5°; field of view (FOV), 180 × 180 mm2; matrix, 150 × 150; section thickness, 1.2 mm; number of excitations, 1.0; bandwidth, 31.2 kHz; and acquisition time, 5.5–6.5 min. The scan parameters of three-dimensional TOF-MRA were as follows: TR, 20 ms; TE, 3.4 ms; flip angle, 16°; FOV, 200 × 200 mm2; matrix, 384 × 224; section thickness, 1.0 mm; number of slices, 180; number of excitations, 0.85; bandwidth, 50.0 kHz; and acquisition time, 4 min 40 s (3 slabs; overlap between slabs, 13 sections; 1 slab, 42 sections).
We measured the absolute signal intensity (SI) and standard deviation (SD) of bypass arteries in both types of MRA and calculated the signal-to-noise ratio (SNR). The region of interest (ROI) was set in the vessel lumen of the developed bypass arteries (Supplemental Fig. 1). The SNR was calculated as the division of SI and SD of the same region of interest (ROI).
DSA of catheter-based intra-arterial cerebral angiography was performed using an AXIOM Artis Zee BA Twin and Artis Icono D-Spin (Siemens Healthcare, Erlangen, Germany).
Statistical analysisThe maximum intensity projection image scores of the two observers were averaged and compared using the Wilcoxon signed-rank test. Weighted κ statistics were used to evaluate inter-observer and intermodality agreement in the direct and indirect bypass development of DSA and the two types of MRA between two observers, which were interpreted as follows: 0, no agreement; 0–0.19, poor agreement; 0.20–0.39, moderate agreement; 0.40–0.59, good agreement; 0.60–0.79, excellent agreement; and 0.80–1.00, almost perfect agreement [16]. Statistical analyses were performed using GraphPad Prism version 7.02 (GraphPad Software, San Diego, CA) and Microsoft Excel (Microsoft, Redmond, WA). P-values of < 0.05 were considered statistically significant.
Comments (0)