
Remember me


The patient was a 51-year-old man. HIV-1 was found to be positive in 2014, and western blot results identified p17, p24, p31, p51, p55, p66, gp41, gp120, and gp160. Highly active antiretroviral therapy (HAART) with undetectable viral load was immediately started. In 2021, the patient developed erythema and scaling on the face and lower limbs, recurrent rash, and no involvement of nails or joints. He had been diagnosed with psoriasis at another hospital, and the rash subsided after 1 month of oral cyclosporine treatment. Due to concerns about cyclosporine-induced nephrotoxicity, hypertension, and especially suppression of T-cell immunity, cyclosporine was discontinued one month later, and the patient's condition recurred. In November 2023, he came to the clinic, and the patient's skin lesions were mainly distributed on the face (Fig. 1), which seriously affected the patient's social life, self-confidence, and quality of life. Baseline hematology and metabolic laboratory results were normal. HBsAg, HBsAb, HBeAg, HCV-Ab, and T-SPOT were negative, HBeAb and HBcAb were positive, and HBV DNA was < 100.00 IU/mL. The Counts of CD4 T lymphocyte and CD8 T lymphocyte were 641 cells/ μl and 654 cells/μl, respectively, the CD4/CD8 ratio was 0.8, and HIV viral load was not detected. No infections were found in the lungs, digestive tract, and other areas. In the context of anti-HIV therapy, 160 mg of Ixekizumab was administered subcutaneously at week 0, followed by 80 mg at weeks 2, 4, 6, 8, 10, and 12, and then maintained at 80 mg every 4 weeks. The patient's skin lesions were completely cleared at week 10 and currently maintained on Ixekizumab for seven months with no episodes of skin lesions observed (Fig. 2). Laboratory data in June 2024 showed a CD4 T lymphocyte count of 618 cells/μL, a CD8 T lymphocyte count of 609 cells/μL, the CD4/CD8 ratio was 1.02, and HIV viral load was not detected (Table 1). No infection was found.
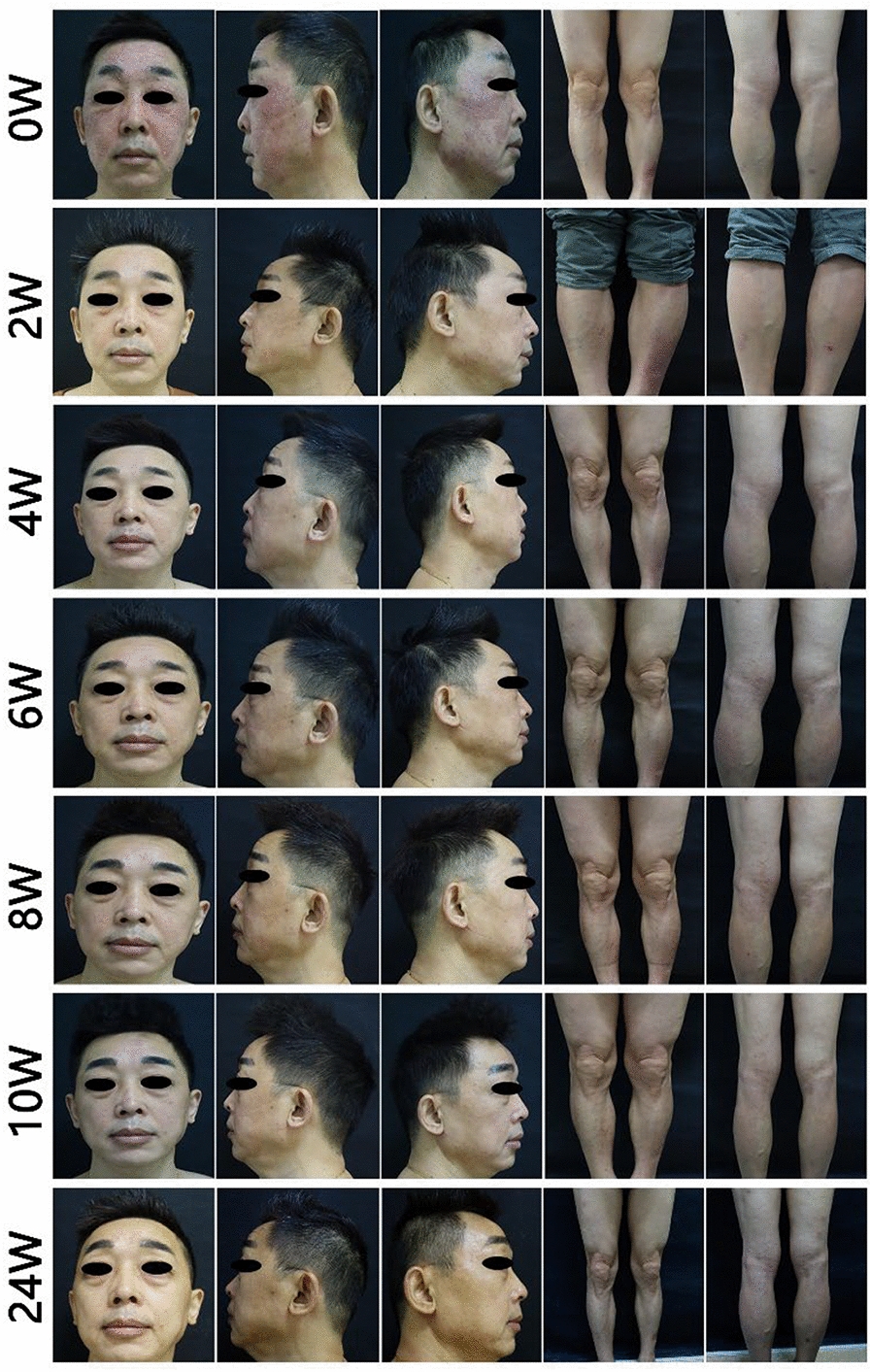
Fig. 1
Ixekizumab treatment photographs. Ixekizumab treatment started (erythema and thin scales distributed on the face and lower legs), the second week (facial erythema and scales significantly subsided), the fourth week (complete clearance of facial lesions, fading color of leg erythema, and reduction of scales), the sixth week (complete clearance of lesions), the eighth week (no new onset of facial rashes, small patchy erythematous patches on the lower legs), and the tenth week (complete clearance of rashes, and lasts until week 24 with no new onset were found)
Fig. 2
PASI Score for Ixekizumab Treatment
Table 1 HIV parameters (CD4, CD8, and viral load) before and during Ixekizumab
Comments (0)