Novel findings and clinical implications
In our study, HIV patients exhibited an increased risk of developing uveitis. When categorizing the various subtypes of uveitis, elevated risks were consistently observed across different follow-up intervals, except for anterior uveitis. The risk of uveitis among HIV patients was present regardless of gender, race, or age (specifically those younger than 70 years). Furthermore, individuals presenting with AIDS symptoms had a higher risk of uveitis compared to those with asymptomatic HIV infection. Notably, the likelihood of uveitis in HIV patients remained elevated even among those who had initiated HIV treatment within three months.
The relationship between uveitis and HIV is increasingly recognized in several case series [1, 11, 13, 16, 24]. The etiology of uveitis in people living with HIV (PLWH) may be multifactorial. Therefore, it is essential to raise awareness about uveitis and its clinical presentations among both HIV-infected patients and healthcare professionals specializing in infectious diseases. To the best of our knowledge, this is currently the only large-scale, multicenter cohort study that extensively investigates the relationship between these two conditions. Besides raising awareness of uveitis in PLWH, our study provides clinical insights into uveitis development in those patients initiating HIV treatment.
Significant findings compared to existing literature
Building on the foundation of previous studies, our research demonstrated that PLWH and those diagnosed with AIDS face higher risks of uveitis. Yen et al. conducted a cohort study to determine the association of HIV with incident uveitis through the Taiwan Centers for Disease Control (TCDC) HIV Surveillance Database [15]. Besides the authors’ conclusion that HIV infection serves as an independent risk factor for the development of incident uveitis, our findings point out the profound immunosuppression associated with this increased risk. A hazard ratio of 5.42 was obtained in their study, which was higher than that of ours. Notably, the authors did not elaborate on their exclusion criteria for HIV-associated diseases. In addition to receiving a uveitis diagnostic code before inclusion in the study, it is important to consider the reported co-infections associated with HIV infections and their respective disease statuses [5]. In previous retrospective case series, the anterior segment was the most prevalent form of uveitis among PLWH [11]. Under the same study design, Makunyane et al. reported that ocular manifestations were slightly more prevalent in the posterior segment than in the anterior segment [18]. However, the design introduces several biases, as opportunistic infections may also play a role in the development of uveitis. In contrast, our research used a cohort study design to calculate the hazard ratio. We found the risk of developing anterior uveitis was not statistically significant until the three-year follow-up period. This indicates that current findings based on case series are not robust enough and warrant further validation using a more rigorous study design.
The advent of ART has significantly improved survival rates for PLWH, leading to changes in the ocular manifestations associated with the infection. Before the implementation of ART, CMV retinitis was the most common ocular complication of HIV [9]. However, its incidence has diminished by over 95% following the introduction of ART [23]. However, it still remains the most common opportunistic infection in HIV even in the ART era [6, 25]. The consistently elevated risk observed across different follow-up intervals in terms of intermediate and posterior uveitis, as well as panuveitis, reinforces the previous statement. Furthermore, the numerical data are consistent with the epidemiological findings, indicating that most of our uveitis events are classified as intermediate and posterior uveitis subtypes, whereas the incidence of anterior uveitis is marginally lower than that of panuveitis (Table 2).
We found that the risk of uveitis remained consistently high in patients initiating HIV treatment within three months. To avoid confusion with opportunistic infections, we specifically excluded the two diseases most likely to cause infectious uveitis—syphilis and tuberculosis to discuss the increased likelihood of uveitis in the absence of other infections. Interestingly, previous research by Kunavisarut et al. found all patients with HIV-induced uveitis demonstrated improvement with ART [10]. Their populations exhibited a lower likelihood of co-infections, as there were no signs or laboratory evidence of syphilis or tuberculosis diagnoses during the patient recruitment. Our study’s strength lies in using large-scale cohorts to validate their findings. The initial population setting was similar to theirs; however, the risk of uveitis persisted even when starting relative HIV treatment. While the initiation of HIV treatments may alleviate current ocular inflammation, the underlying risks remain. We hypothesize that the immune response may react to other underlying pathogens after recovering from HIV treatment. Several studies on immune reconstitution inflammatory syndrome (IRIS) support our hypothesis [5, 8, 20, 22, 25].
Possible explanations underlying the observed results
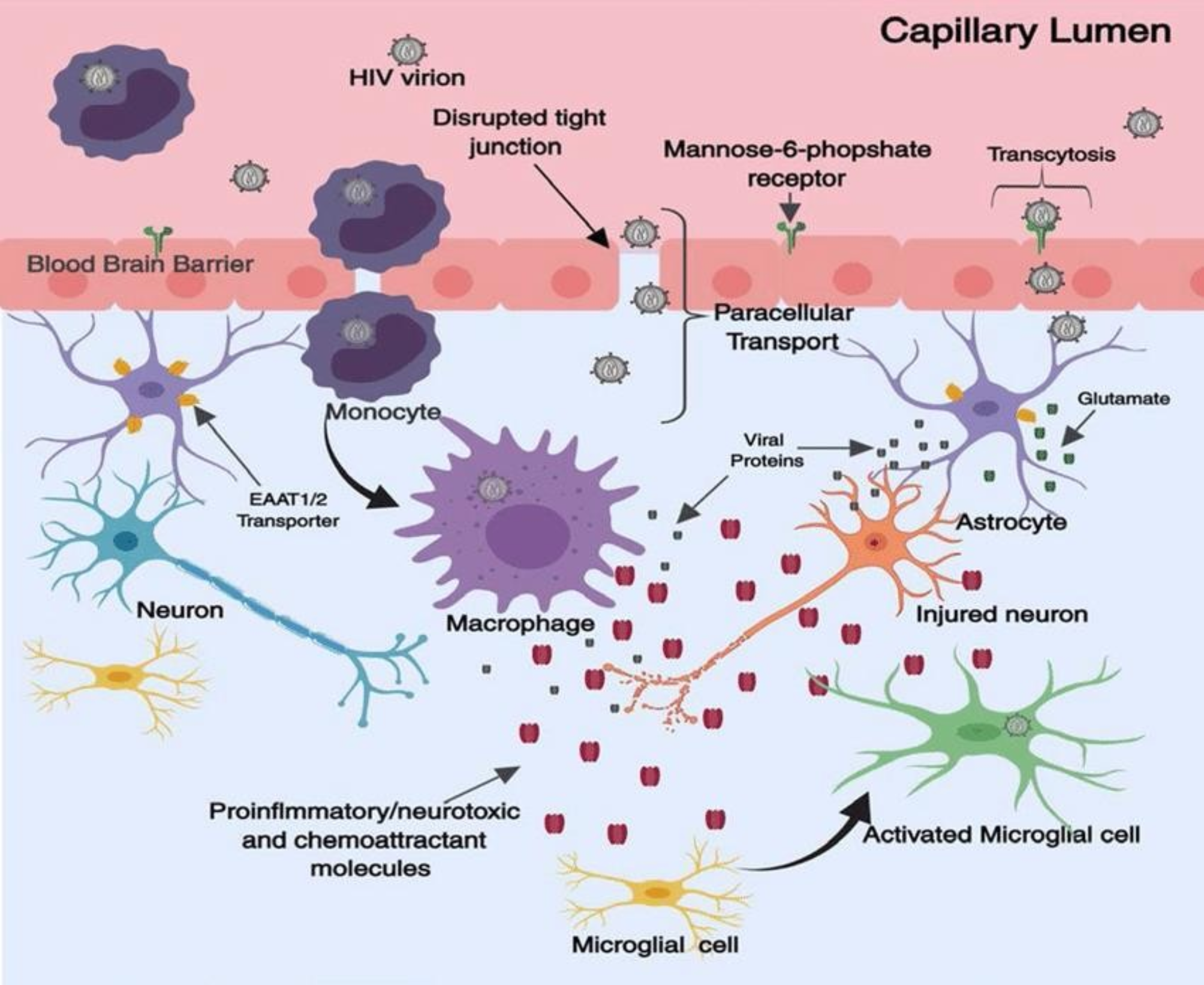
HIV-associated uveitis has been extensively documented in recent studies, which have demonstrated that HIV can infiltrate the central nervous system and replicate within ocular tissues [14, 26, 27]. Pathanapitoon et al. revealed intraocular HIV viral load was detectable in uveitis patients with HIV, with some cases showing higher levels in the eye than in plasma [28]. From an immunological perspective, the depletion of CD4 + T cells induced by HIV, along with subsequent opportunistic infections and co-infections, has contributed to an increased prevalence of uveitis as a complication related to HIV [12]. Although previous work did not identify a correlation between CD4 + T cells and intraocular viral loads [28], we believe the immune response may elucidate the heightened risks of uveitis development observed in our research.
ART has been linked to a higher incidence of IRIS, with immune recovery uveitis (IRU) being a common ocular manifestation. IRU occurs when new inflammatory processes emerge in an eye previously affected by controlled CMV retinitis or other opportunistic infections, with no alternative etiology identified, after significant immune recovery [21]. The exact pathogenesis of IRU remains incompletely understood. It has been partially attributed to the presence of autoreactive T lymphocytes that arise during the immune reconstitution process in predisposed individuals [19]. A previous multicenter cross-sectional study indicated that patients with HIV and CMV retinitis who experience immune recovery are at a significant risk of developing IRU [29]. The occurrence of uveitis is thought to be associated with CMV infection, particularly given the rarity of IRU in non-CMV eyes [21]. Our findings support this assertion. The sensitivity analysis specifically conducted for uveitis after HIV treatment (Table 5) indicates that, upon excluding CMV infection, a risk reduction is observed, thereby substantiating the relationship between CMV infection and HIV-induced uveitis. Notably, our study’s most significant finding is that, even after excluding CMV infection populations, the risk of uveitis remains elevated compared to that of the general population three months post-HIV treatment. In the era of ART, it is commonly accepted that ocular complications significantly decrease after CD4 cell count recovery. However, our study calls into question the validity of this assumption. We propose several potential explanations for this discrepancy. First, many opportunistic viral infections, such as HSV and VZV, can cause uveitis. Nevertheless, due to the invasive nature of polymerase chain reaction (PCR) testing, these infections may not consistently be captured in the diagnostic codes during follow-up assessments. Second, the primary parameter for monitoring ART is the CD4 cell count. Although a three-month treatment period is anticipated to yield favorable outcomes according to established guidelines, the lack of CD4 cell count data complicates the definitive assessment of HIV infection control after only three months of treatment, which may serve as indirect evidence. Another aspect to consider is from the perspective of IRU, suggesting that a form of immune dysregulation is likely caused by improper reconstitution of systemic immune cells. The observed imbalance in effector and regulatory T cell reconstitution contributes to excessive inflammatory responses in HIV patients undergoing ART [30]. The reduced number of Th17 cells and weak antiviral CD4 + T cell responses noted in IRU patients further exemplify a compromised immune recovery when compared to those without IRU [31]. Additionally, the presence of specific cytokines, such as IL-12, with reduced levels of IL-6 and the absence of CMV replication in the eyes of IRU patients [32], underpins the distinctive immune imbalance inherent in IRU’s pathophysiology. We advocate for further research focusing on the immunological aspects, in addition to investigating any underlying pathogens in PLWH.
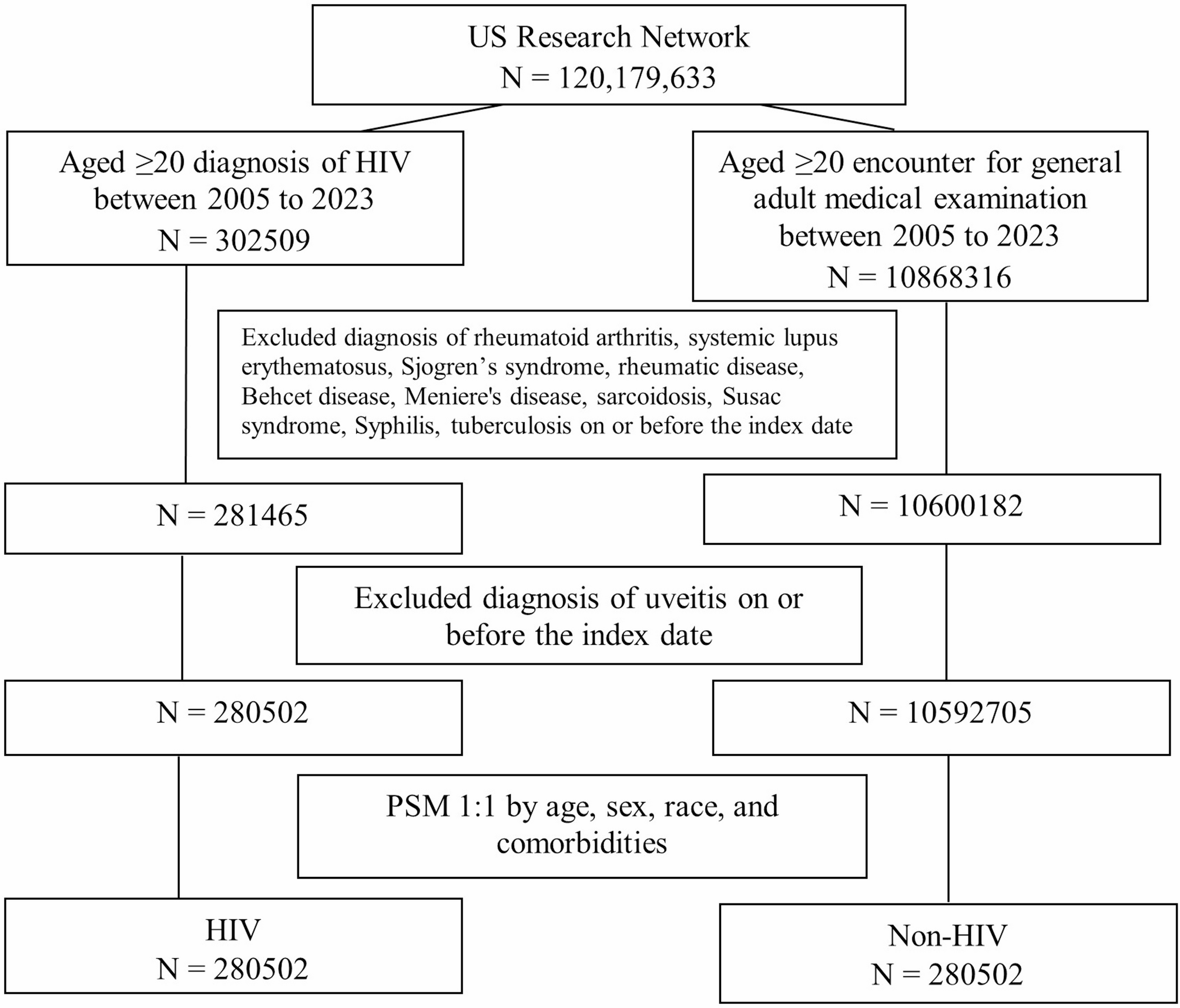
Another ocular manifestation known as drug-related uveitis is primarily associated with cidofovir and rifabutin [33,34,35]. However, these two medications are not utilized in our HIV treatment regimen (Table S2). Therefore, this type of uveitis is less likely to account for the increased risk of uveitis observed in HIV patients undergoing treatment within three months. Regarding uveitis due to co-infections, we excluded common opportunistic infections associated with HIV, such as syphilitic uveitis and tuberculous uveitis in our study; however, a heightened risk of uveitis among PLWH was still noted. We attribute these findings primarily to previous CMV infections, which continue to represent one of this population’s most frequent ocular complications.
Limitations
Our study has several limitations that should be acknowledged. Firstly, due to the retrospective cohort design, a causal relationship could not be established in HIV patients receiving related treatments. Secondly, the relatively small number of events in our study, especially in follow-up interval strata, may significantly reduce the power of our statistical tests. The variability within the small sample size could mask the true effect, making it challenging to reach statistical significance. Thirdly, when evaluating ocular side effects caused by HIV infection, the CD4 cell count is often critical. CD4 + counts of less than 200 cells/µL are generally considered to indicate a high risk. Our analyses did not include subgrouping of related immunological cell counts and cytokine concentrations due to the lack of definitive clarifications in this area. Furthermore, this study did not include additional adjustments for borderline-balanced or unmeasured variables in our Cox regression model because the function was not available in TriNetX database. The potential for unmeasured confounding could affect our results because of the pathophysiological nature of HIV infection.



Comments (0)