
Remember me


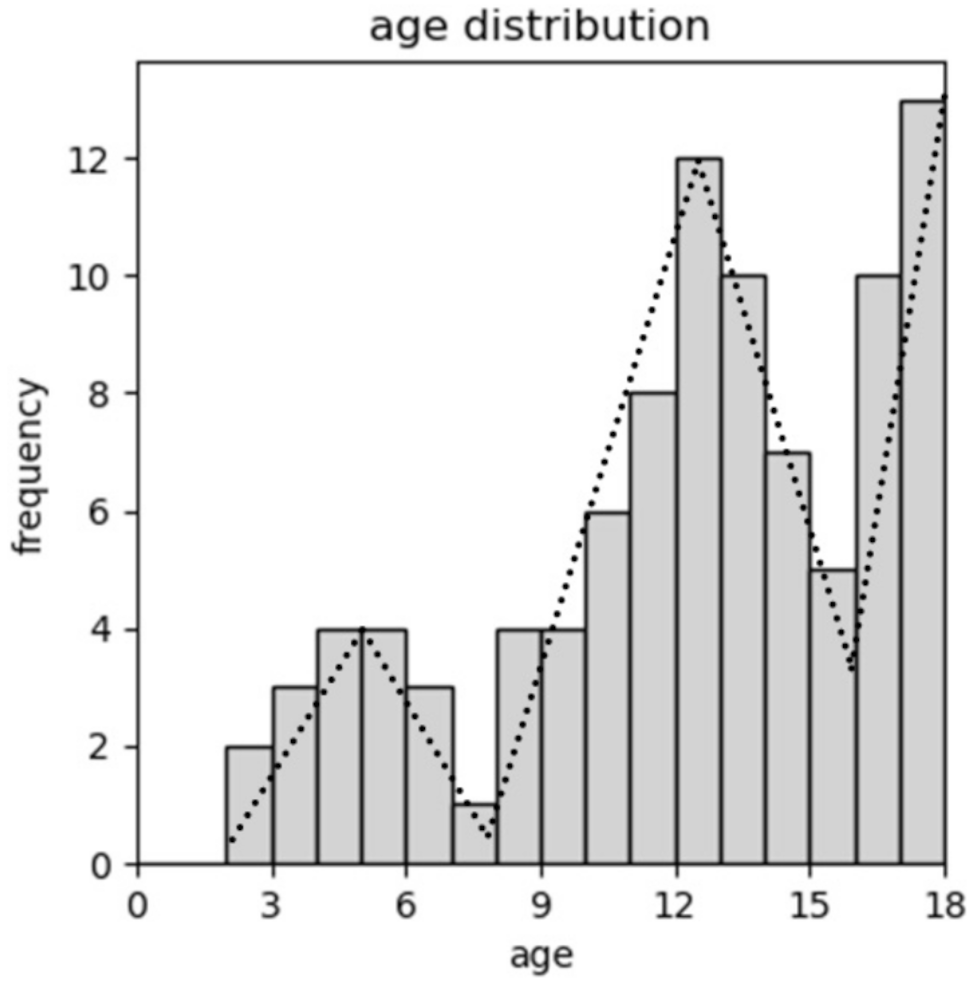


Out of 133 identified patients with paediatric uveitis between January 2012 and June 2022, 96 patients (56/93 with initial bilateral diseases, total of 149 affected eyes) could be included in the study. Median age at first presentation at our clinic was 12.0 years (range 2.0 to 17.6 years). There is a three-peaked age distribution with a first peak in preschool, a second peak in early teens, and a third in late teens as illustrated in Fig. 1. No female / male difference was found with 51% compared to 49%, respectively. Non-infectious etiology was apparent in more than double compared to infectious causes with 68% compared to 32%, respectively. Anterior uveitis was most common documented (50%), followed by posterior (28%), intermediate (20%), and panuveitis (2%). The overall most common etiology was toxoplasmosis (20%), followed by JIA (8%) and suspected herpetic infection (8%). Two female patients, both presenting with intermediate uveitis at age 17 years, were later (2 months and 2 years) diagnosed with multiple sclerosis (MS). One female patient with papillitis, 7 years of age, was diagnosed with tick-born encephalitis (TBE), confirmed by lumbar puncture. This child was not vaccinated. She presented complete recovery from the TBE. Another female’s anterior uveitis, presenting at 5 years of age, was preceded by salmonella diarrhea. It was considered to be a reactive uveitis and treated with topical steroids only, as the diarrhea has spontaneously ceased and there was no sign of invasive disease. Other associations were Susac syndrome (female, 17 years old), TINU syndrome (male, 13 years old), systemic lupus erythematodes (female, 15 years old), Crohn’s disease (male, 11 years old), ankylosing spondylarthritis (female, 13 years old), and familial Mediterranean fever (male, 12 years old) as summarized in Fig. 2.
Fig. 1
Age distribution at first presentation. There is a three peak distribution, with a first peak in preschool, a second in early teens, and a third in late adolescence
Fig. 2
Piechart of uveitis etiologies or associated diseases. Infectious causes made up nearly one third, with toxoplasmosis being the most frequent etiology, followed by herpetic diseases. Other infectious causes were tick-born encephalitis, chlamydia urethritis, and gastrointestinal salmonella. 69% were found to be non-infectious uveitis, with 44% of unknown cause (whereof 11% were ANA positive and 5% were HLA B27 positive), 8% were JIA associated uveitis, 2% were later diagnosed with multiple sclerosis. Other associated diseases were Susac syndrome, TINU, SLE, Crohn’s disease, ankylosing spondylitis, familial Mediterranean fever. One patients was had a masquerade syndrome with ALL. INF, infectious; ANA, antinuclear antibodies; HLA, human leukocyte antigen; JIA, juvenile idiopathic arthritis; MS, multiple sclerosis; TINU, tubulointerstitial nephritis uveitis syndrome; SLE, systemic lupus erythematodes; ANCA, anti-neutrophil cytoplasmic antibodies; ALL, acute lymphoblastic leukemia
One patient at age 13 years had a masquerade syndrome secondary to preexisting, still active acute lymphoblastic leukemia (ALL). No associated infectious cause or systemic disease was found in 44% of the cases, thereof 11% had elevated ANA and 5% tested positive HLA B27 (to note that HLA B27 tests were only documented in 60% of the patients). ANA patterns were analysed in eleven patients. In this sub cohort, no association between ANA pattern and systemic disease was found.
The distribution of associated diseases differed between the affected segments: Anterior uveitis was mostly associated with non-infectious causes (80%) whereas intermediate uveitis was always associated with non-infectious causes. Posterior uveitis was mostly of infectious cause with 81%. In contrast, panuveitis was always of non-infectious cause (see Table 1). Further, bilateral disease was strongly associated with non-infectious uveitis (93% of the cases), whereas unilateral disease was more likely to be of an infectious cause (70% of the cases), with an odds ratio of 31 (95% confidence interval 9–106) (see Table 2).
Table 1 Distribution of infectious and non-infectious uveitis according to the primarily involved segmentTable 2 Cross-tabulation of laterality versus infectious and non-infectious uveitisMean VA at first presentation of affected eyes was 0.79 (range hand motion to 1.6) and mean IOP was 13.6mmHg (range 5.5 to 28.0). VA was significantly worse in cases with infectious uveitis compared to non-infectious uveitis (0.64 versus 0.83, p = 0.017, Mann-Whitney-U test). There was no significant difference in IOP.
Complications were documented in nearly one third of all affected eyes (see Table 3). This included optic disc swelling (18%), synechiae (10%), cataract (5%), band keratopathy (3%), epiretinal membrane (2%), macula edema (1%), retinal neovascularisations (6%) and vitreous hemorrhage (1%). IOP was above 21 mmHg in five eyes at first presentation (3%). No patient presented with clinically significant hypotony. The overall presence of complications did not differ between in non-infectious and infectious uveitis cases (28% versus 29%). Complications affecting the anterior segment were more prevalent in non-infectious uveitis. In contrast, complications affecting the posterior segment were more prevalent in infectious uveitis, but without clinical significance when adjusting for the distribution of affected segments in infectious and non-infectious uveitis.
Table 3 Complications at first presentationSymptoms expressed by the patients were documented in 88%. This included blurred vision (26%), floaters (19%), photophobia (17%), and headache (7%). A redness of the eye was noted by the patients or guardians in 39%. There was no significant difference in incidence of complications between the patients with or without complaints.
Comments (0)