This dose-expansion cohort evaluated safety and efficacy of mosunetuzumab in Japanese patients with R/R FL and ≥ 2 prior lines of therapy. Fixed-duration mosunetuzumab induced a high ORR and CRR with a manageable safety profile. Safety and efficacy data from this analysis were consistent with that previously reported in the global phase I/II GO29781 study [10, 11].
The follow-up period of this analysis was shorter than the global study (8.0 months vs 18.3 months); however, the proportion of patients who completed eight cycles of treatment after achieving CR at C8 was similar [11]. In this analysis, mosunetuzumab demonstrated a high CRR (68.4%) and ORR (78.9%), including a high CRR in patients with POD24 (80.0%), and response to treatment was observed regardless of prior therapy and refractoriness. In one patient who had received prior CAR-T, CR following mosunetuzumab treatment was observed, with no CRS. While CRRs were similar across subgroups, the small number of patients in each subgroup limits the reliability of these comparisons. Eleven (57.9%) patients did not experience POD24. Both DoR and DoCR at 6 months were consistent with the results of the global study [10, 11]; however, due to limited follow-up, it is necessary to interpret the median values with caution. Due to the limited number of patients, no firm conclusions for PFS or OS can be made.
Overall, mosunetuzumab monotherapy demonstrated a manageable safety profile. The AE profile and severity of AEs were consistent with the known safety profile of mosunetuzumab [8,9,10,11]. Of note, a higher incidence of Grade 3–4 AEs was reported in this analysis versus the global phase I/II GO29781 study [10, 11]. This could be attributed to the difference in incidence of lymphocyte count decreased/lymphopenia, which is associated with the mode of action of mosunetuzumab, and unlike this analysis was not frequently reported in the global study.
The incidence of AEs leading to mosunetuzumab discontinuation was low. (n = 2; 10.5%), and only one Grade 5 (fatal) AE, which was considered unrelated to mosunetuzumab, was reported. The rate of neutropenia/neutrophil count decrease was comparable between this and the global study (26.3% and 28.9%, respectively) [11]. The current trial was held during the COVID pandemic, and one serious event of COVID-19 pneumonia was reported; no febrile neutropenia events and no Grade 5 (fatal) AEs due to infection were reported. Neurological AEs consistent with ICANS were rare in both studies, one patient in the current study and 1% of patients (Grade 1: 0.5%; Grade 2: 0.5%) who received mosunetuzumab at the recommended dose in the global trial [11]. Overall, no new safety findings were observed, which was expected given the tolerable mosunetuzumab dosing regimen established in the global phase I/II GO29781 study [10, 11].
The incidence of CRS was similar between this and the global phase I/II GO29781 study, with any-grade CRS events observed in 47.4% and 44.4% of patients, respectively [11]. Most CRS events in this study were Grade 1 (36.8%) and were lower grade versus the global study, with steroids as the premedication for CRS at C1 and C2 in both studies [11]. Consistent with the global study, responses to treatment were observed in patients regardless of whether they experienced a CRS event [11]. This suggests that the use of SUD decreased the risk of CRS, while CRS events do not influence the clinical efficacy of mosunetuzumab. The use of tocilizumab and steroids to mitigate CRS was comparable between the two studies.
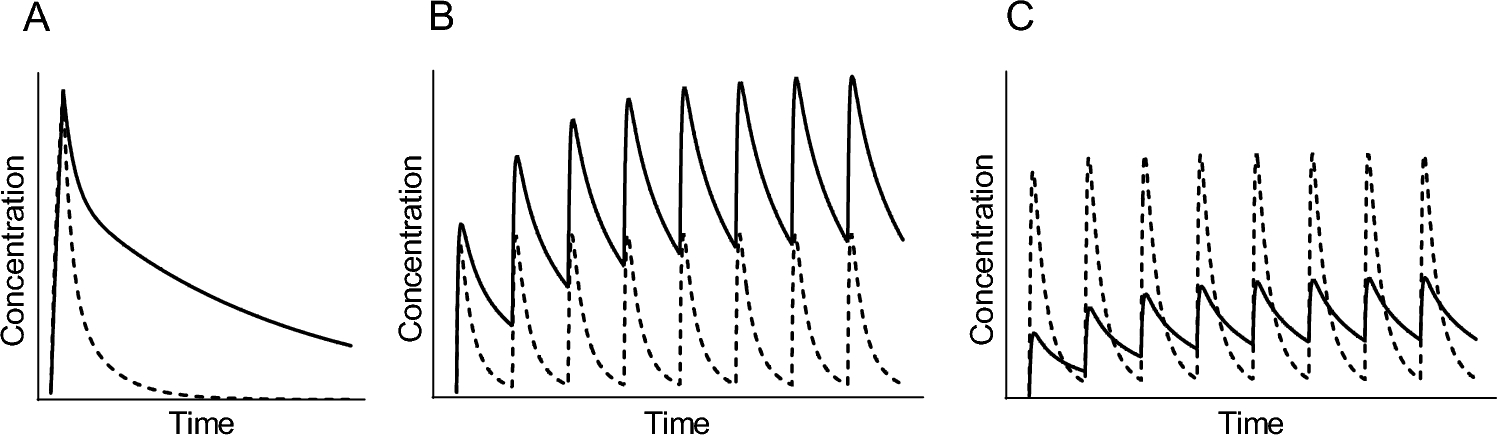
The blood concentration of mosunetuzumab increased in a dose-dependent manner in this study [13]. While the half-life of mosunetuzumab was not evaluated in this dose-expansion cohort due to limited blood sampling points, the apparent half-life of the first dosing for Japanese patients has been previously reported [13]. The mean Cmax (CV%) and mean AUC (CV%) at the RP2D were 26.2 μg/mL (27.8%) and 345 (26.5%) day*μg/mL, respectively, compared with 17.9 μg/mL (49.6%) and 246 (46.9%) day*μg/mL, respectively, at the same RP2D in Group B in the global phase I/II study [18]. Although a trend toward higher exposure was observed in this analysis compared with the global phase I/II GO29781 study, the differences observed are likely due to the difference in body weight between the two studies. Pharmacokinetic data in this dose-expansion cohort are consistent with those observed in the Japanese Phase I study [13].
In the current study, the correlation between response and peripheral T cells was not investigated; however, no association between baseline B cell, T cell, or NK-cell counts, and response was observed in the global phase I/II GO29781 study [11].
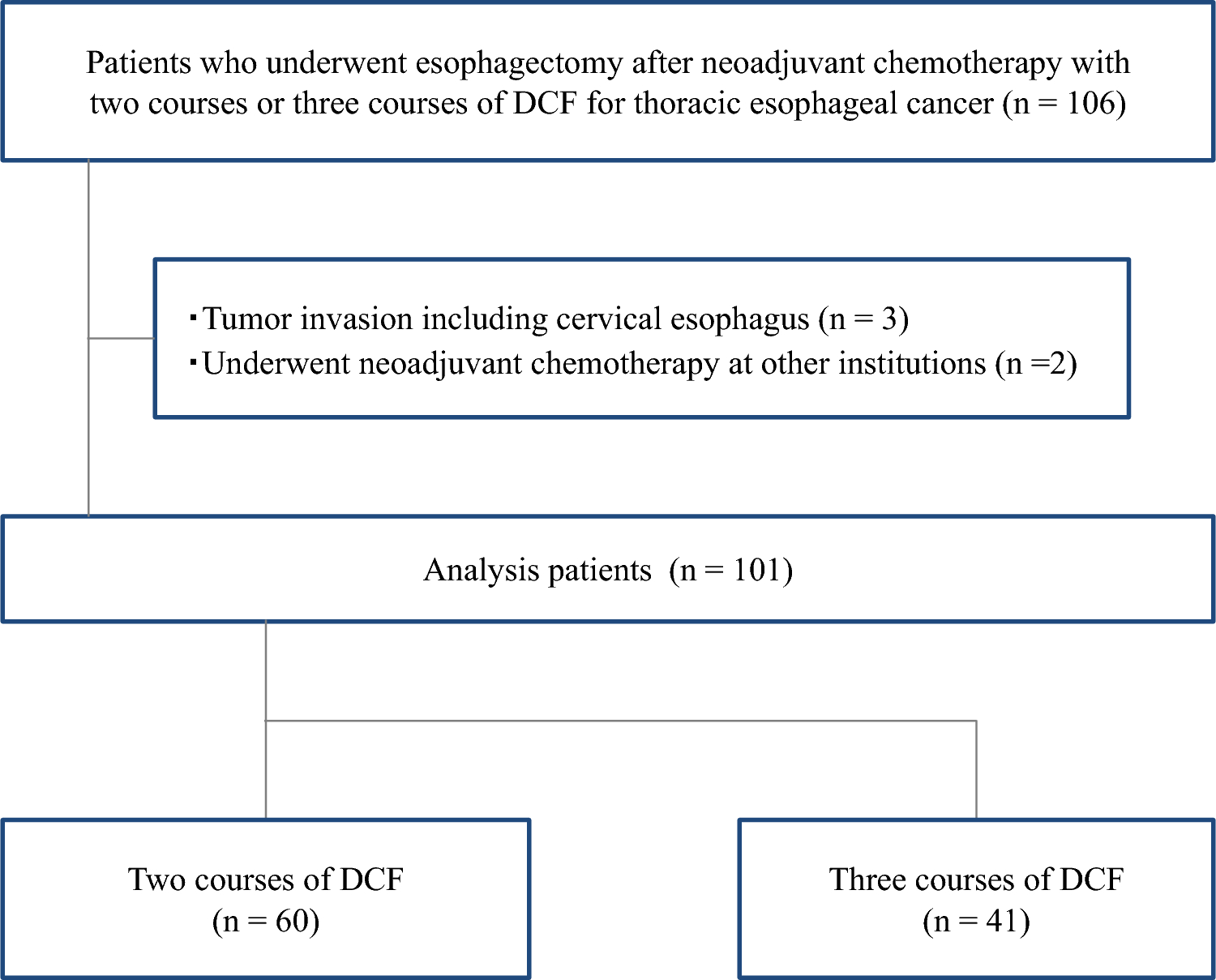
Limitations of this analysis include a lack of control group and the small number of Japanese patients enrolled (N = 19). The duration of follow-up in this study was relatively short (8.0 months); however, results from the global phase I/II GO29781 study, with longer follow-up, demonstrate efficacy of mosunetuzumab treatment with a long DoR and manageable safety [11].
Given the lack of clear evidence for treating 3L + FL with various treatments, including CAR-T, in clinical practice, prolonged follow-up of mosunetuzumab may be considered for future studies to extend upon the efficacy findings of this analysis.

Comments (0)