Systematic literature search
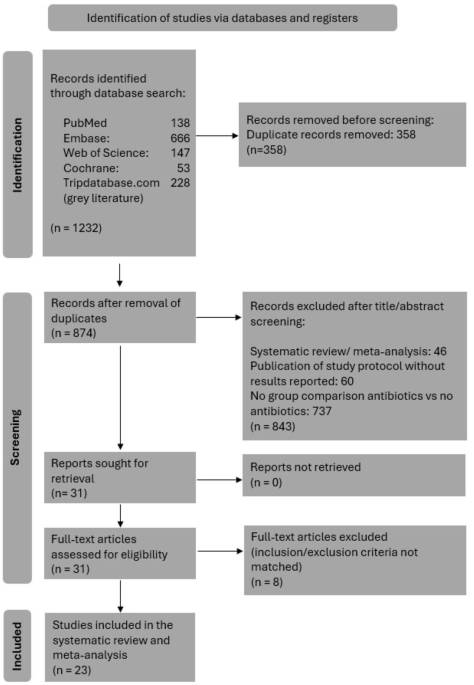
Relevant RCTs evaluating 1 L treatments in men ≥18 years with asymptomatic or mildly symptomatic mCRPC were identified via a systematic literature review (SLR) following established best practices [6, 11]. The protocol was registered with the International Prospective Register of Systematic Reviews (registration number: CRD42021283512).
The search strategy was developed and tested by a medical information specialist in consultation with the review team and peer-reviewed independently by another senior medical information specialist using the Peer Review of Electronic Search Strategies (PRESS) checklist. The following electronic databases were searched using the Ovid® search interface: Embase, Ovid MEDLINE® (including Epub Ahead of Print and In-Process & Other Non-Indexed Citations), Ovid MEDLINE® Daily, Cochrane Central Register of Controlled Trials, and the Cochrane Database of Systematic Reviews. These searches were performed on September 9, 2021, and updates of these searches were performed on February 17, 2022, and October 3, 2022.
Websites of key clinical conferences were hand searched for relevant abstracts from 2019 to 2022. Grey literature searches of key clinical conferences, the US National Institutes of Health (NIH) ClinicalTrials.gov, Food and Drug Administration (FDA), European Medicines Agency (EMA), and reference lists of previously published reviews were conducted. Key HTA agencies (National Institute for Health and Care Excellence [NICE], Canadian Agency for Drugs and Technologies in Health [CADTH], and Scottish Medicines Agency [SMC]) were also hand searched for relevant technology appraisals.
Title and abstract screening against pre-defined eligibility criteria was performed in duplicate by two reviewers using DistillerSR [7]. After initial screening, full-text articles were obtained for potentially eligible citations and reviewed by two reviewers to determine formal inclusion. Reasons for exclusion were documented at the full-text stage. Any screening discrepancies between the two reviewers were resolved by consensus or by a third independent reviewer. Detailed study eligibility criteria is available in Supplementary Appendix A. Data extraction was performed by one reviewer and validated by a second reviewer using data extraction templates in Microsoft® Excel (Microsoft Corporation, Seattle, US). Data elements captured during extraction included publication characteristics, study setting, study methods, study participants, and study findings. The risk of bias assessment was performed using the NICE Single Technology Appraisal Evidence Submission Checklist for assessment of risk of bias in RCTs [12].
Feasibility assessment
To ensure sensible and robust comparisons in the indirect treatment analysis, the similarity of included studies of interest was qualitatively assessed. Between-study heterogeneity was conducted for the following elements: trial design and methodology, baseline patient characteristics, trial eligibility criteria, outcome assessments, interventions, comparators, and their contribution to a connected network (i.e., a common comparator).
Outcomes
Outcomes assessed in this analysis included rPFS as assessed by blinded independent central review (BICR), overall survival (OS), PFS on the next line of therapy (PFS2), time to prostate-specific antigen (PSA) progression, time to cytotoxic chemotherapy initiation, PSA response, and objective response rate (ORR).
Statistical analysisMatching-adjusted Indirect comparison
Given the lack of a common comparator between TALAPRO-2 and PROpel, and TALAPRO-2 and MAGNITUDE, unanchored MAICs were conducted to estimate the relative treatment effect of TALA + ENZA versus OLAP + AAP, and NIRA + AAP by leveraging IPD from TALAPRO-2 (all-comers for comparisons with PROpel and HRRm for comparisons with MAGNITUDE) and published aggregate data from PROpel (all-comers) and MAGNITUDE (HRRm).
The phase 3 TALAPRO-2 trial was assessing TALA + ENZA as 1 L treatment in patients with mCRPC in two cohorts: Cohort 1, the all-comers cohort and Cohort 2, HRR-deficient only for DNA damage response alterations in genes directly or indirectly involved in HRR [4]. The most recent data cutoff (DCO) for TALAPRO-2 Cohort 1 (DCO: 28/03/23 for OS and DCO: 16/08/22 for all other outcomes) and TALAPRO-2 Cohort 2 (DCO: 03/10/22 for all outcomes) were used for the present analysis. Analysis of comparator studies also used the most mature data identified in the searches. For the PROpel trial, this analysis used results based on DCO 12/10/22 for OS and PFS2 [13], DCO 14/03/22 for ORR [14], and DCO 30/07/21 for rPFS (BICR) and PSA response [8]. For the MAGNITUDE trial, this analysis used results based on DCO 17/06/2022 for rPFS (BICR), OS and time to cytotoxic chemotherapy [10] and DCO 8/10/2021 for both time to PSA progression and ORR [15]. Note, data for TALA + ENZA was provided by Pfizer at the time of review given the TALAPRO-2 trial was ongoing. Since the last SLR update conducted in October 2022, results for the TALAPRO-2 trial have been published (DCO: 16/08/22) [4]. Updated OS data (DCO: 28/03/23) for TALAPRO-2 used in the present analysis were provided by Pfizer (confidential, data on file). Updated data for PROpel [13] and MAGNITUDE [16], and additional information from the full-text publications for MAGNITUDE were incorporated into the analyses. Data were derived from aggregate data for PROpel and MAGNITUDE by reconstructing reported data for PSA response and ORR, and by simulating IPD for rPFS, OS, PFS2, time to PSA progression, and time to cytotoxic chemotherapy initiation from digitized published Kaplan-Meier (KM) curves using the Guyot method [17,18,19].
The TALAPRO-2 population was adjusted to match the eligibility criteria and distribution of prognostic and treatment effect-modifying factors between study populations. Patients from TALAPRO-2 who did not fulfill the eligibility criteria of the comparator study were removed to better align the two populations. Patients from TALAPRO-2 who satisfied the eligibility criteria of PROpel and MAGNITUDE, respectively, were reweighted to adjust for imbalances in baseline characteristics of prognostic significance (see Appendix B). Factors predictive of the treatment effect of therapies in mCRPC were identified through the literature [20] and clinical expertise and were ranked in order of importance by an experienced clinician (see Supplementary Table 2). Population differences between TALAPRO-2 and the comparator studies were assessed using standardized mean differences (SMDs), where an SMD between 0 and 0.1 was considered a small difference, an SMD > 0.1 and ≤0.2 was a moderate difference, and an SMD of >0.2 was a substantial difference [21].
A form of propensity score weighting was used, in which patients in TALAPRO-2 were weighted by the inverse odds of being in that group compared to the other group based on the values of their baseline characteristics. Weights were based on a generalized method-of-moments propensity score algorithm, which guaranteed a close balancing of covariates between TALAPRO-2 and PROpel populations, and TALAPRO-2 and MAGNITUDE populations [22, 23]. Results of the TALAPRO-2 study were reanalyzed using the weighted patient-level dataset. Treatment outcomes were then compared across balanced study populations.
The effective sample size (ESS) was calculated to reflect the impact of weighting on the available information in the IPD [22]. The ESS is the number of non-weighted patients that would produce a treatment effect estimate with the same precision as the reweighted sample estimate. Since these MAIC analyses provided an unanchored indirect comparison due to the lack of a common comparator arm in each comparison, all treatment effect modifiers and prognostic variables should be adjusted to ensure balance and reduce bias [22].
For time-to-event outcomes (i.e., rPFS, OS, PFS2, time to PSA progression, time to cytotoxic chemotherapy initiation), hazard ratios (HRs) were estimated using a weighted Cox proportional hazards model. For response outcomes (i.e., PSA response, ORR) odds ratios (ORs) were estimated using a weighted generalized linear regression model using a binomial likelihood and logit link function. The corresponding variances were estimated using a robust sandwich estimator, and 95% confidence intervals (CIs) were reported.
Validity of the proportional hazards assumption for rPFS, OS, PFS2, time to PSA progression, and time to cytotoxic chemotherapy initiation was assessed using the Grambsch-Therneau test [24] (with a p-value less than. 05 considered to indicate a violation of the assumption).
Additional unanchored MAICs for rPFS and OS were conducted to estimate the relative treatment effects between the control arm from TALAPRO-2 (ENZA, all-comers) using IPD and both the active and control arms from PROpel (OLAP + AAP and abiraterone acetate plus placebo [AAP + PBO]) using published aggregate data as well as TALA + ENZA (TALAPRO-2) versus AAP + PBO (PROpel). Similarly, unanchored MAICs for rPFS and OS were conducted to estimate the relative treatment effects between the control arm from TALAPRO-2 Cohort 2 (ENZA) using IPD and both the active and control arms from MAGNITUDE (NIRA + AAP and AAP + PBO) as well as TALA + ENZA (TALAPRO-2 Cohort 2) versus AAP + PBO (MAGNITUDE). The same statistical methodology as described above was applied for these analyses. All analyses were conducted using R version 4.1.2 (R Core Team, Vienna, Austria) based on the methods developed by Signorovitch et al. [25], and as implemented by the National Institute for Health and Care Excellence (NICE) Decision Support Unit Technical Support Document series [26].
Sensitivity analysis
Sensitivity analyses were conducted to investigate the impact on the treatment effect estimates, ESS, and SMD when adjusting for additional covariates in the analysis. A series of sensitivity analyses were conducted whereby all commonly available rank-ordered variables were sequentially and incrementally adjusted for until the final model contained all available factors.
Exploratory analysis
In addition to the twelve prognostic factors identified which informed the primary analysis, four additional covariates were identified as variables of interest (i.e., BRCA1, BRCA2, BRCA co-occurring, and PALB2), based on clinical opinion. A series of exploratory analyses were also conducted whereby these additional factors were sequentially and incrementally adjusted for.




Comments (0)