Study and procedures
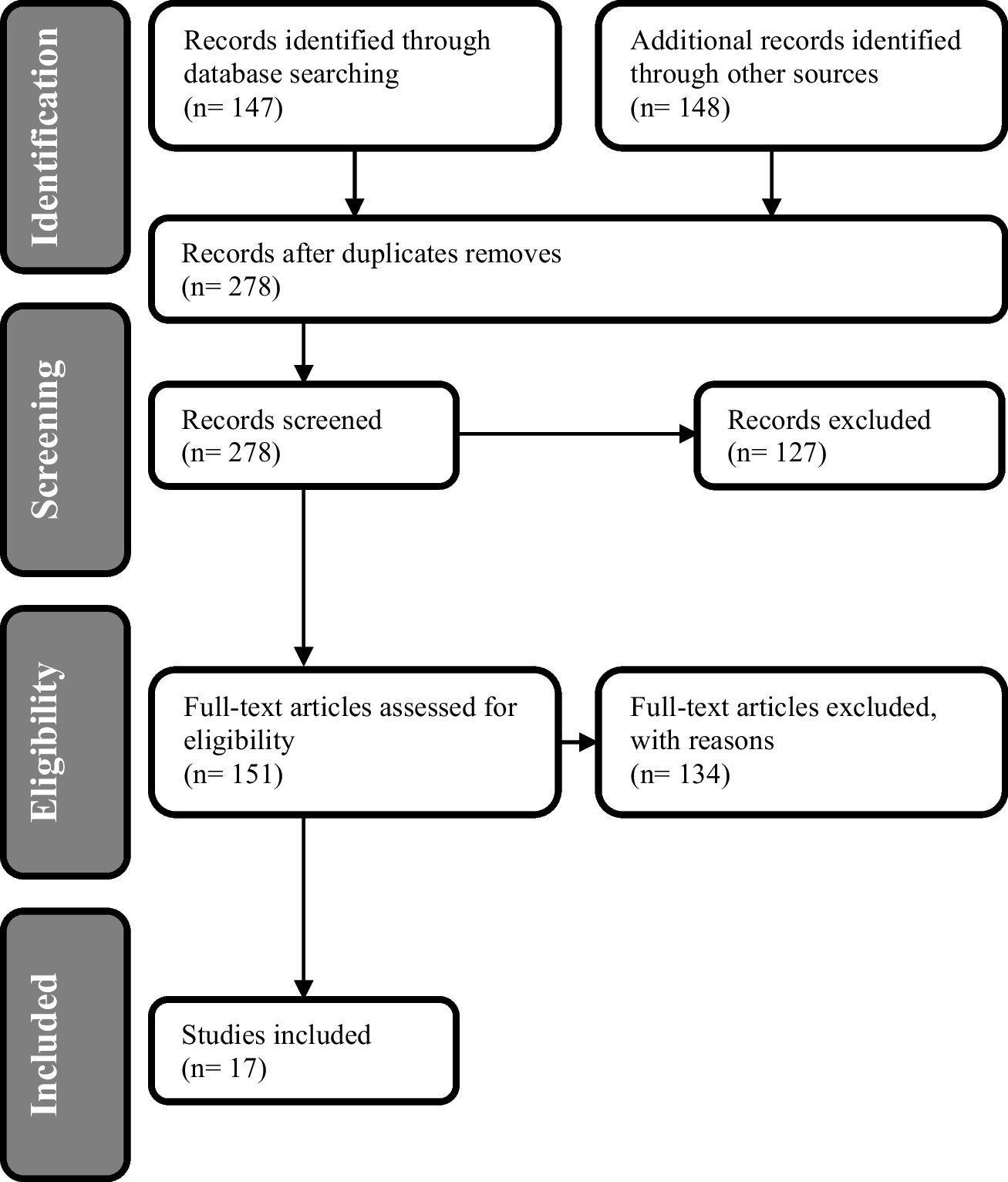
Data were collected in the survey on study conditions and mental health of university students (acronym StudiBiFra), a nationwide collaborative project between Charité – Universitätsmedizin Berlin and Bielefeld University in which cross-sectional online surveys were conducted between June 2021 and March 2023 at 13 German universities. From the 13 universities, 3 were universities of applied sciences. Throughout this article, the term “university” refers to both universities and universities of applied sciences. Participating universities were from eight different German federal states (Alice Salomon University of Applied Sciences Berlin, Aschaffenburg University of Applied Sciences, Charité – Universitätsmedizin Berlin, Heidelberg University of Education, Heinrich Heine University Düsseldorf, Humboldt University of Berlin, Ilmenau University of Technology, Martin Luther University Halle-Wittenberg, Technical University Braunschweig, University of Applied Sciences and Arts Dortmund, University of Applied Sciences Münster, University of Cologne, University of Rostock). Students at each university were invited to participate via email, websites, flyers, and social media, among other channels, with each university managing the recruitment process. Prior to the start of the survey, which was implemented in LimeSurvey (LimeSurvey GmbH, Hamburg, Germany), all students gave their informed consent to participate and could choose to complete the survey in German or English (with the exception of one university which conducted the survey in German only). This study was performed in line with the principles of the Declaration of Helsinki. The Ethics Committee of Charité – Universitätsmedizin Berlin approved the study (Date: 26.03.2021/ No. EA1/055/21).
Questionnaire and measures
The Bielefeld Questionnaire on Study Conditions and Mental Health was used, which is based on the framework of the Bielefeld Company Model and thus the Bielefeld Social Capital Approach (Badura et al. 2013). According to this approach, organisational conditions named “drivers” have impact on dimensions of mental health and well-being, which are referred to as “outcomes”. The drivers include, in particular, social resources of the organisation (referred to as “social capital”) like the quality of leadership, the quality of collaboration, and the shared values of the organisation (organisational culture) (Badura et al. 2013). Based on this framework, the Bielefeld Questionnaire on Working Conditions and Health in Higher Education Organisations was developed and subsequently adapted to students as members of universities as the Bielefeld Questionnaire on Study Conditions and Mental Health (Burian et al. 2019a). The questionnaire was validated and pretested at one faculty at Bielefeld University (n = 264 participants) (Burian et al. 2019b).
Socio-demographic variables
Students were asked to indicate their gender identity, selecting from three options (“female”, “male”, and “gender-diverse”) or to provide “no answer” for this item. Every university was asked to insert their own list of study programmes. In order to aggregate the data, students were grouped into five categories: education, humanities, social, behavioural and media sciences, economics, law, languages, arts, and culture (“humanities”) (1), natural and life sciences, mathematics, and statistics (“natural sciences”) (2), engineering, technology, and architecture (“engineering”) (3), medicine and health sciences (“health”) (4), and “other” (5). The variable “type of university” differentiated between “universities” (1) and “universities of applied sciences” (2). Students who were in their first or second semester were classified into the category “first year of study” (1), students who agreed to the statement “I will finish my studies this or next semester.” Were classified into the category “last year of study” (3), and all other cases were categorised as “all other semesters” (2).
Assessment of study conditions
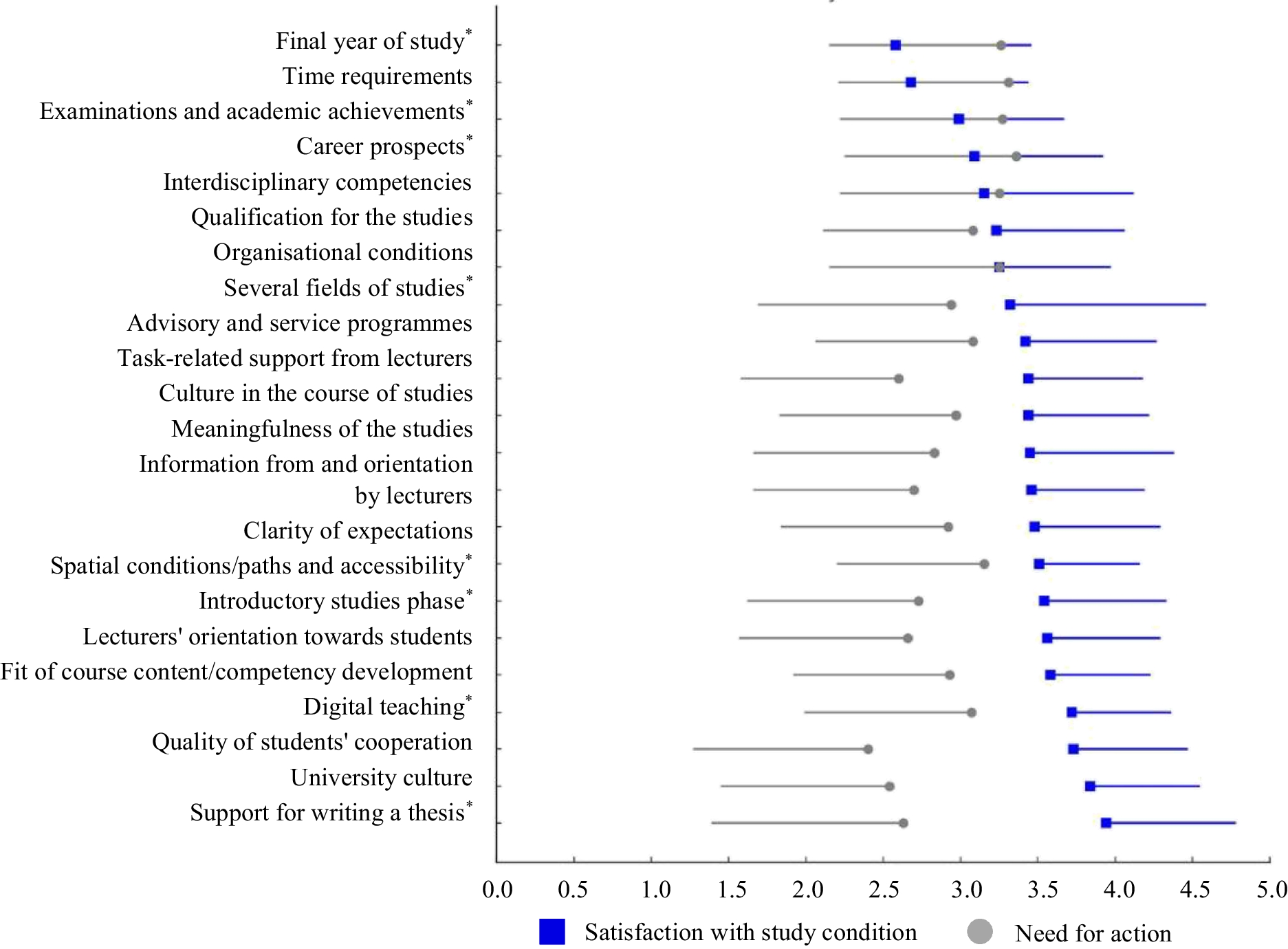
Study conditions were assessed in 22 different thematic domains (e.g. time requirements and university culture). Each domain was evaluated through a battery of 1–14 items. Each item consisted of a positively or negatively formulated statement (e.g. “In my studies, I have to manage too many things at once.” or “Appropriate breaks are planned between the courses.”) with a corresponding 5-point Likert-type response option (e.g. “strongly agree” to “strongly disagree” or “very satisfied” to “very dissatisfied”). Agreement with positively formulated statements or disagreement with negatively formulated statements were considered as satisfaction with the current condition. Some items of study conditions were only allocated to students to whom they apply. For instance, all items of the domains “spatial conditions/paths and accessibility” and one item from the domain “organisational conditions” were answered only by students who reported attending (at least partially) face-to-face courses. A complete list of the items regarding study conditions, their filters and reliability data can be found in Appendix 1.
Scale means for each domain of study conditions were calculated. Missing values in any item of the domain were person-mean imputed by the mean of the remaining items of the respective scale, if the number of missing items was below one-third of the number of items in the domain, following Robinson (2018). If more than one-third of the items of the respective scale were missing, no mean value was calculated.
Measurement of the needs for action
Following each thematic domain of study conditions, students were asked to state how urgently the university should address the issue in question in order to provide universities with information for priority preventive actions. The needs for action were formulated as follows: “How urgently should [our university] address the issue of [study condition domain]?”, and answers ranged from “no need for action at all” to “very great need for action” on a 5-point Likert-type scale.
Mental health and well-being variables
Mental health was measured with four scales: general well-being (3 items), depressive symptoms (5 items), cognitive stress symptoms (4 items), and exhaustion (3 items). All mental health statements were assessed using the following question “How often did the following statements apply to you during the last two months of your studies?”. Answer options ranged on a 5-point Likert-type scale from “(almost) always” to “(almost) never”.
General well-being: While one item within the general well-being scale was developed specifically for this study, the remaining two were derived from the “Productivity and Social Capital in Business” (ProSoB) questionnaire (Badura et al. 2013). Cronbach’s α for this scale is 0.80.
Depressive symptoms: The five items measuring depressive symptoms originated from the ProSoB questionnaire (Badura et al. 2013). Cronbach’s α for this scale is 0.90.
Cognitive stress symptoms: The four items evaluating cognitive stress symptoms sourced from the “Copenhagen Psychosocial Questionnaire” (COPSOQ) (Nübling et al. 2006). Cronbach’s α for this scale is 0.86.
Exhaustion: The three items for exhaustion were adapted from the ProSoB questionnaire (Badura et al. 2013). Cronbach’s α for this scale is 0.76.
Scale means for each mental health scale were calculated. Missing values in any item of the domain were replaced by the mean of the remaining items of the respective scale, if the number of missing items was below one-third of the number of items in the domain. If more than one-third of the items of the respective scale were missing, no mean value was calculated.
Mental health problems: In addition, the four scale means of mental health variables were combined into an overall variable for mental health problems by creating a mean of the four mental health mean scores for cases with scale means for all four mental health variables. In order to create the overall mental health problems variable, the general well-being scale was inversely coded. Consequently, higher values of the resulting mean (max. 5) indicated higher levels mental health problems, while a mean of 1 represented the lowest possible level of mental health problems. A complete list of the items of the mental health scales is provided in Appendix 2.
Statistical analysis
Frequencies for categorical and means with standard deviation for numeric variables were calculated. To analyse differences in satisfaction with study conditions and needs for action by field of study, gender identity, study phase, and type of university, t-tests and analyses of variance (ANOVAs) were calculated.
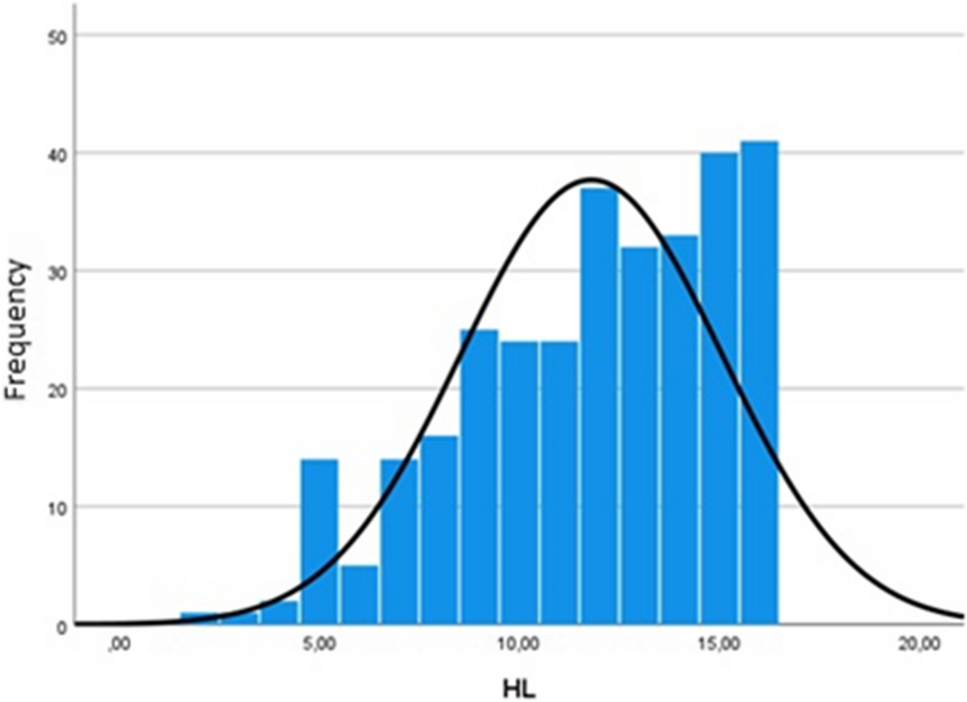
Subsequently, five sets of linear regression analyses were performed for the variable overall mental health problems as well as for all four single aspects of students’ mental health (general well-being, depressive symptoms, cognitive stress symptoms, and exhaustion) as dependent variables. Scale means of all 22 thematic domains of study conditions served as independent variables. Field of study, gender identity, institution, and study phase were included as categorical covariates. Before computing the linear regressions, the requirements were checked: The single mental health variables and the overall mental health problems variable were considered normally distributed. Multicollinearity was not apparent in our models (VIF 1.01 to 1.16). In the context of this study, regression coefficients up to 0.10 are considered low, from over 0.10 to 0.30 as moderate, and above 0.30 as high associations (analogous for negative associations). A Bonferroni-adjusted alpha level of 0.2% was used to evaluate the significance for detected associations.

Comments (0)