The large variation in workplace support for sick-listed employees that we observe among countries and welfare regimes points to deep-rooted differences in institutions and policy approaches. On a general level, we can link the involvement of employers in facilitating RTW to the features of the different welfare models.
The Nordic countries have a long tradition of active labour market policies and striving for high employment rates. In Sweden, active labour market policy measures were first implemented in the post-war decades as part of the Rehn-Meidner model of economic policy (Morel et al. 2012). While the other Nordic countries do not have such a long history of activation measures, they all tend to score high in comparisons of different indicators aimed at capturing the intensity of activating labour market policies (Martin 2015). The strong orientation towards promoting employment is also reflected in the high activity rates of older workers in these countries, which we can interpret as a proxy for the labour market inclusion of persons with health limitations. In 2019, against an average employment rate for 55–64 year olds of 58.6% in the European Union, the Nordic countries had employment rates between 65.9% (Finland) and 76.5% (Sweden).
The Liberal welfare regime, with its emphasis on means-tested social benefits and strong reliance on market-based solutions, is often portrayed as the antithesis of the Scandinavian model. In this respect, it may seem surprising at first glance that workplaces in countries associated with these very different welfare regimes have similarly high RTW support rates. However, the prevalence of RTW support in countries such as Ireland and the UK is consistent with an institutional set-up in which the management of sickness absences is left mainly to private actors, with comparatively little state involvement. In contrast, the low level of employer involvement in Southern and Eastern Europe is consistent with systems of welfare provision that are less developed or rely heavily on the role of families. A comparison of disability policy models in Europe has highlighted that Southern European countries are part of a policy cluster characterized by an emphasis on social protection rather than labour-market integration, while most Eastern European countries have comparatively low levels of both social protection and integration measures (Tschanz and Staub 2017).
It is interesting to note that the distribution of RTW procedures by welfare regimes corresponds broadly to the ranking of European countries according to the Active Ageing Index (AAI). The AAI is a measure of policies that support the potential for active and healthy ageing among older people and was developed for the European Commission and the United Nations Economic Commission for Europe (Zaidi et al. 2013). The countries associated with the Nordic and with the Liberal welfare models score high on the AAI, while Eastern and Southern European countries score particularly low. Research on active ageing has singled out especially Eastern European countries as late movers in the implementation of policies to promote healthy ageing (Naegele and Bauknecht 2019).
The degree of employer involvement in the different RTW phases is clearly also affected by specific sick-leave policies and institutions (de Rijk et al. 2020). Also in this respect, there is a strong correspondence between policies and the levels of employer support for RTW that we observe across welfare regimes. A study by EU-OSHA shows that Eastern European and Southern European countries have only “limited” or “ad hoc” frameworks for rehabilitation and RTW, which are either focused exclusively on workers who have formally been recognised as disabled, or lack coordination mechanisms between stakeholders to ensure RTW (EU-OSHA 2016). The Nordic countries (as well as Germany and Austria), on the other hand, have comprehensive RTW systems, targeting all workers and aiming to prevent exclusion from the labour market through prevention, early intervention and coordination between stakeholders.
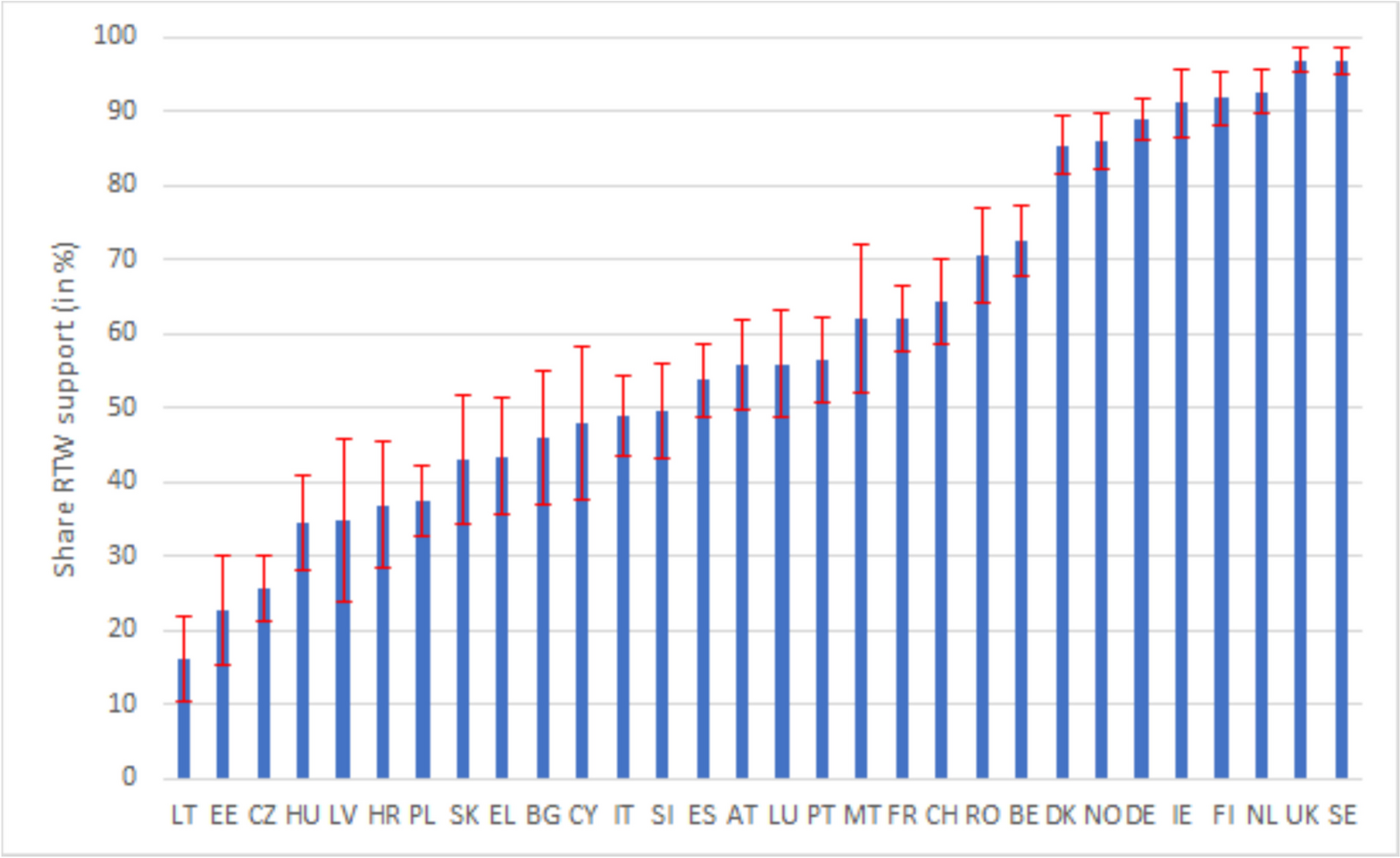
Despite these broadly consistent patterns between welfare regimes, we must not overlook elements of heterogeneity, both in the form of outliers in RTW support within clusters and in the form of differences in policies between countries with similar prevalence of RTW procedures. Outliers concern, for instance, the high RTW support rate in Germany within the Continental cluster or the comparatively low prevalence in Switzerland within the Liberal cluster. On the other hand, countries with similar rates of workplace support for sick-listed employees are sometimes characterized by very different policies and institutional arrangements. This is particularly evident when we look at the group of countries with the highest diffusion of RTW procedures, i.e. the Nordic and Anglo-Saxon countries together with Germany. Employers’ actions are influenced by regulations on managing sickness absences but also by economic incentives, such as the amount and duration of wage replacement during sick leave, known as the employer period. These elements, which together form what has been termed the “follow-up regime for sick-listed employees”, determine how the responsibility and the financial burden of sickness absence is shared between the social protection system, employers and employees in each country (Ose et al. 2022).
In countries with extensive legislation and policies on sickness absence, mutual investment in RTW efforts is expected by both the employer and the worker, and employers tend to have a clear understanding of their duties (de Rijk et al. 2020). This is predominantly the case in the Nordic countries, although the specific institutional set-up differs considerably from country to country (Clayton et al. 2012; Hemmings and Prinz 2020; Ose et al. 2022; Leoni 2022). Norway and Sweden have a relatively short employer period, followed by a long public-funded sickness benefit. However, in the event of a prolonged sick-leave, employers are required to become active and prepare a return-to-work or rehabilitation plan. In Denmark, the wage payment regulations are similar to those in Sweden and Norway, but municipal job centres play the central role in sick-leave follow-up, whereas in Finland the occupational health services (OHS) have an important role in sickness absence management and employers have only limited duties.
Although the employer periods are short, in all these countries employers may have additional incentives to engage in RTW activities because often individual contracts or collective agreements provide for more generous wage payments during sick-leave. The economic incentives to help sick-listed employees in their return to the workplace are even greater in the Netherlands, where employers have to cover income replacement for their employees during the first 2 years of sick leave. In addition, Dutch employers have strict requirements in promoting rehabilitation and return-to-work, which is why the Netherlands can be singled out as the country with the strongest combination of legal requirements and high financial costs associated with sick-leave. In the UK, which ranks among the countries with the highest RTW shares, employers do not have any obligations towards their employees with respect to the follow-up of sickness absences, but they bear most of the sickness absence costs (with an employer period of up to 28 weeks) and may therefore have high incentives to reduce absences. In Germany, which according to the ESENER data is the only representative of the Continental welfare regime to have a large diffusion of RTW procedures, the employer period is of intermediate length (6 weeks) but, in cases when the sick leave lasts longer than 6 weeks, employers have to contact their employees and offer support for their return-to-work.
Strengths and limitations
Despite the growing consensus on the central role that workplaces and employers should play in efforts to extend working lives, there is a gap in comparative research on the prevalence of employer activities to facilitate RTW. This study contributes to closing this gap, providing fine-grained and robust evidence on RTW procedures in workplaces across a large set of European countries. This evidence provides a suitable basis for generating and testing new hypotheses, including the role that specific policies but also institutional interdependencies and welfare state characteristics play as determining factors of employer engagement in RTW efforts.
There are, however, several limitations, mainly related to the imperfect measurement of employer activity in sickness absence follow-up in the data used. Smaller establishments are not included in the more recent ESENER waves and there are limitations in data comparability across waves. Moreover, information on the existence of workplace procedures to support RTW is binary, and the data do not tell us whether these policies are applied to the whole workforce or only to selected segments. Similar RTW-support shares may thus mask differences in the share of the labour force that is covered by these policies, as employers may differentiate between worker categories (for instance, between workers with temporary and permanent contracts). It is also important to acknowledge that the results presented in this study are not suitable for drawing conclusions about whether differences in employer support for RTW lead to higher retention rates and improved employment outcomes for sick-listed workers.
Future research
Currently, there is little evidence on the way in which different institutions, regulations and incentives affect employer behaviour in the management of sickness absences and in efforts to promote the return of sick-listed employees to their workplace. In this respect, comparative studies using quantitative approaches could be just as useful as detailed comparisons between individual countries or smaller groups of countries. We also need to better understand whether and to what extent differences in employer responsibilities influence the employment outcomes of workers affected by a health shock or the onset of a chronic illness. Data simultaneously providing information on both sides of the employment relationship as well as on health and other individual characteristics should be applied to investigate causal mechanisms.

Comments (0)