Ameloblastic carcinomas are rare entities that may pose diagnostic dilemmas [1, 3], particularly in distinguishing cases with intermediate histopathologic features. This difficulty is further exacerbated by poorly defined diagnostic thresholds [7]. Further studies are required to better elucidate this entity and improve the diagnostic work-up of potential cases.
The current study of 29 cases of AC represents a sizeable single-centre study, albeit in the same population group. In this study, the mean age of presentation was 43 years, lower than a recent systematic review [8]. Interestingly, the mean age of primary and secondary ACs was similar. The current study also included a control cohort of ABs, which presented at a comparatively younger age, but was similar to a large single-centre study on ABs within the same population group [10]. ACs showed a male predominance in the current study, contradicting the reported literature [8]. Of note, in the current study, the sample of ABs that transformed into ACs only presented in male patients. Due to the relatively small sample, this finding should be viewed cautiously. As expected, the median clinical duration of tumours in the current study was markedly higher for secondary AC cases than for primary cases.
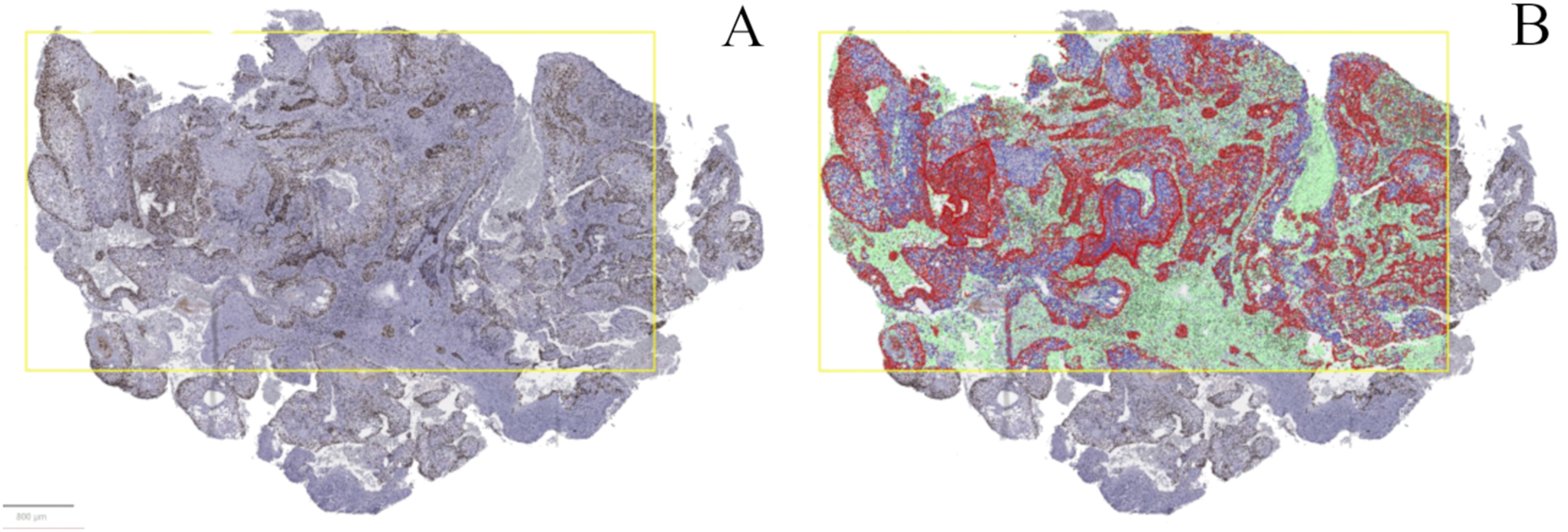
Determining the proliferative index of a tumour using Ki-67 IHC has been used as an ancillary tool to differentiate entities with similar histopathologic appearances [4, 11,12,13]. The limitation of Ki-67 IHC revolves around its interpretation and the subjective nature thereof. A recent systematic review recorded a vast range of Ki-67 scores, between 5 and 80% [8]. Regardless of this limitation, literature constantly quotes higher mean proliferation indices in ACs compared to ABs [6, 34]. The findings of the current study mirrored the literature, finding a statistically significant higher Ki-67 score in cases of AC compared to ABs included in the study [9]. A noteworthy difference in the current study stemmed from using an automated proliferation index counter, thereby increasing the number of cells analysed and reducing the subjective nature and reported range in interpreting the IHC stain.
Tumour neoplastic cells, in particular malignancies, are known to contain DNA content changes and cell cycle variations [14]. Utilising this principle, cytometric measurements of nuclear DNA content by FC have helped distinguish benign and malignant neoplasms [25, 26, 35]. Additionally, measuring DNA by FC may serve as a valuable adjunct to histopathologic evaluation when grading tumours [23, 26]. The nuclear content of several carcinomas, including ovarian, breast, thyroid, and oral, has also provided important prognostic information [36,37,38,39].
Flow cytometry is an accurate, rapid technique to determine the DNA ploidy of individual cells in a suspension [15, 22, 40]. The nuclei are stained with a fluorescent dye and sent through a flow channel, where the dye is excited by a laser beam or mercury lamp. DNA content is measured based on the proportional binding of the DNA-specific dye to nuclear DNA, resulting in a DNA content histogram of the entire cell population [40, 41]. The current study utilised high-resolution FC, whereby DAPI was used instead of the dye propidium iodide. This, linked to the UV light source, produces high-quality histograms [41], as reflected in the current study, which, despite using FFPE tissue, produced an excellent mean coefficient of variance.
Several previous studies have successfully used FC on oral squamous cell carcinomas (SCCs) to correlate DNA ploidy status with tumour grading and staging, tumour progression, recurrence rates and metastatic potential [15, 17, 22, 29, 42, 43]. Salivary gland tumours (SGTs) have also undergone DNA ploidy analysis to distinguish benign versus malignant entities and to correlate with the histopathologic grading of malignant SGTs [14, 21, 23]. Concerning odontogenic lesions, a case report by High et al., utilised FC to determine DNA aneuploidy in an odontogenic keratocyst that underwent malignant transformation. In this case report, the subsequent carcinoma was also aneuploid, both locally and in the metastatic tumour deposit [44]. An early study by Muller et al. utilised image and FC to analyse DNA content in primary and recurrent ABs and AC cases [25]. They analysed 17 primary and five recurrent ABs and five ACs, with fourteen (82%) primary ABs and three (60%) of the recurrent cases being diploid. They found no statistically significant difference in ploidy analysis between primary and recurrent ABs or among the different histological variants included in the study. Importantly four (80%) of the five ACs were aneuploid. FC was performed on three AC cases with 100% concordance between the image and flow cytometric data [25]. The authors concluded that aneuploidy in this tumour group strongly indicates malignancy [25]. This contrasts with the study by Mahmoud et al., in which all eight cases of AC were diploid [27]. More recently, Penafort et al., found that DNA ploidy may act as an ancillary tool in distinguishing AB and AC [28]. Unfortunately, this study included a relatively small sample of five ACs, and DNA ploidy analysis was conducted using conventional FC with propidium iodide dye.
In the current study, almost all ABs within the cohort were diploid, with only a single case of AB that transformed into AC interpreted as aneuploid. Notably, the corresponding AC was also aneuploid. Many authors believe that aneuploidy is a cause rather than the result of malignant transformation, forming an essential part of carcinogenesis. This implies that aneuploidy in tumours at an early stage suggests that abnormal DNA content may be associated with tumour progression [18, 40, 42, 45]. Further studies are required in this regard. Interestingly, in the current study, two cases of AB that transformed into ACs were reported as diploid, with their subsequent corresponding secondary AC being aneuploid. This implies that DNA content changes occurred as part of the malignant transformation. Similar studies on oral SCCs found that aneuploidy formation represents a late but ultimate event in the disease process and contributes to the behaviour of the carcinoma [15, 17, 43]. Another study focusing on genito-urinary neoplasms also found a decrease in the proportion of diploid cases with tumour progression [33].
Regarding primary and secondary ACs, no statistically significant difference was noted between the subtypes of AC and DNA ploidy status, a finding not yet reported in the literature. A significant association was noted when comparing the DNA ploidy status of ABs to ACs. Although not all cases of AC were aneuploid, this affirms the notion by Muller et al. that aneuploidy supports, but is not diagnostic, of malignancy [25]. Tetraploid cells are genomically unstable and known to facilitate tumorigenesis, arising from diploid progenitors by endomitosis and subsequent loss of chromosomes [42, 46, 47]. Additionally, tumour tetraploidy may play a role in tumour progression and relapse following chemotherapeutic treatment [46, 47]. In the current study, only a single case of primary AC showed an aneuploid cell population with tetraploid DNA content, limiting further correlations. Finally, no correlation was noted between DNA ploidy status and Ki-67 proliferation scores for cases of AC in the current study, implying that the two variables are independent features in diagnosing ACs.
A possible pitfall of DNA ploidy analysis by FC is tumour heterogeneity reported in oral SCCs, SGTs and ACs [21, 25, 48, 49]. To counter this drawback, researchers often advocate the repetition of ploidy analysis to exclude spurious diploid cases [21]. Additionally, maintaining excellent CV values, as low as possible, which are reflected on the graph as narrow peaks. This is critical to correctly diagnose diploid cases without missing peridiploid aneuploid peaks, which cannot be detected with high CV values [15]. The mean CV value in the current study was 3.5%, while most studies on oral SCCs using archival material described values higher than 5% when using propidium iodide as a DNA marker [50, 51]. Other studies on DNA FC in odontogenic carcinomas did not reveal the CV values [25,26,27,28], apart from the case report by High et al., which quoted a CV of 7.75% [44]. The use of high-resolution FC in the current study contributed to the excellent reported CV values, despite using FFPE material [29, 30].
The limitations of the current study included the small sample size from a single centre and limited information from clinical records due to the retrospective nature of the study. ACs are rare, highlighting the importance of future collaborative studies to pool all available data for further analyses. Possible case selection bias was mitigated by two oral and maxillofacial pathologists with extensive experience in odontogenic pathology, who confirmed the diagnosis of each case according to the latest diagnostic criteria [3].








Comments (0)