
Remember me


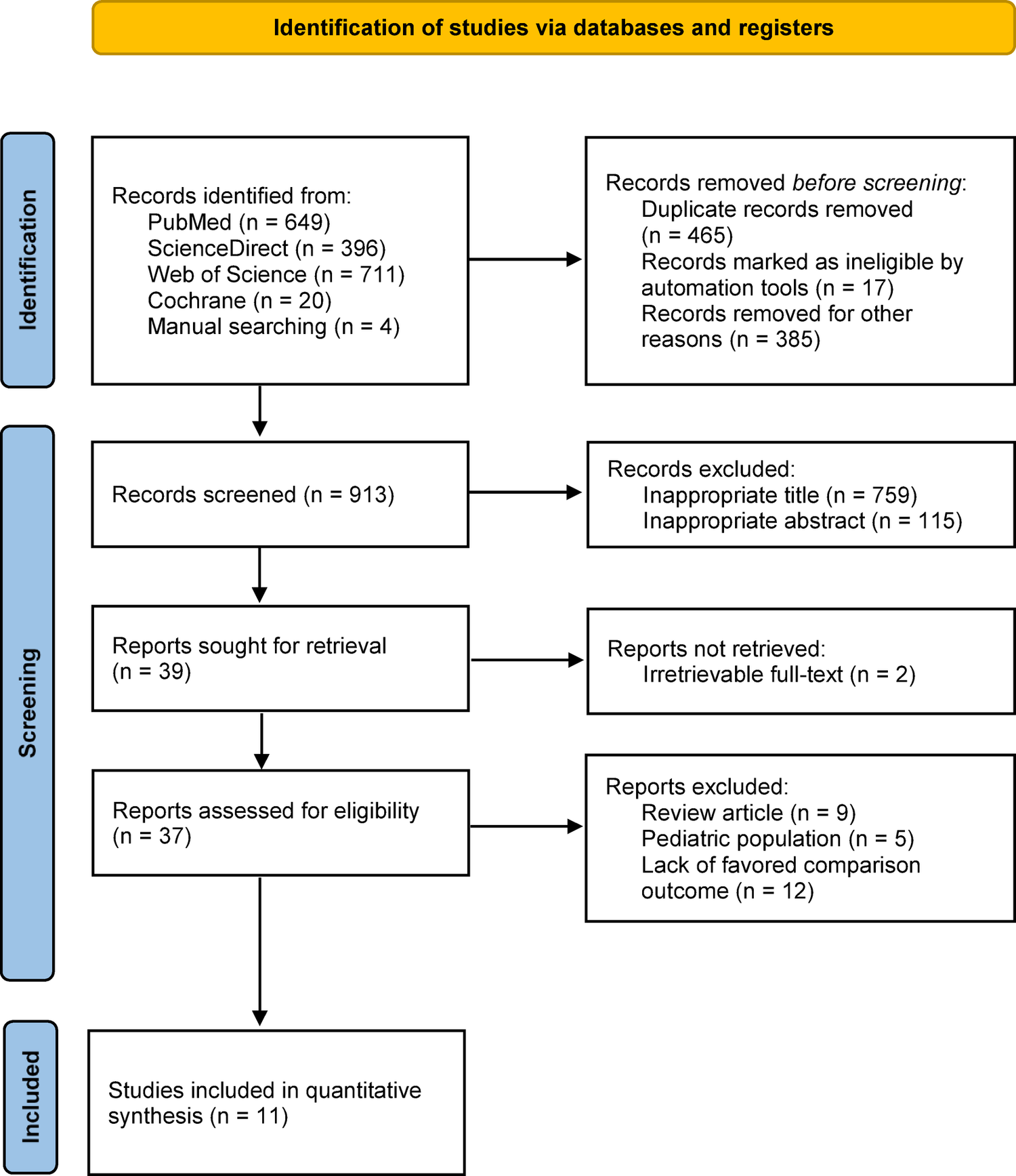
We summarized the study selection process in the PRISMA flowchart (Fig. 1). A total of 760 relevant studies were identified. Of these, 91 studies full-text articles were assessed for eligibility, and 13 studies met our inclusion criteria [17,18,19,20,21,22,23,24,25,26,27,28,29]. Baseline characteristics of the included studies are shown in Tables 2 and 3. Six of the studies were RCTs [18,19,20,21,22,23]. Seven studies were prospective studies [17, 24,25,26,27,28,29]. Seven t studies assessed antibiotic prophylaxis in ULT/URS [18,19,20,21,22,23,24, 27]. Six of the studies assessed antibiotic prophylaxis in PNL [17, 25, 26, 28, 29].
Table 2 Included studies on ureteroscopy (FURS: flexible ureteroscopy)Table 3 Included studies on PCNL (BT: body temperature; HR: heart rate; WBC: white blood cells; NR: not reported; Pts: patients; UC: urine colture; RPUC: renal pelvis urine cultures; SC: stone culture; FT: fosfomycin Tromethamine)Fig. 1
PRISMA flowchart for study selection
Risk of biasFig. 2
We summarized RoB assessment in Fig. 2. Five studies were judged to have low risk of bias [18, 21, 24, 26, 28], five studies at moderate risk of bias [20, 22, 25, 27, 29] and three at high risk of bias [17, 19, 23].
Targeted antibiotic prophylaxis based on preoperative urine cultureWalton et al. [17] conducted a prospective multicenter study to evaluate the concordance of microbiological profiles from preoperative midstream urine culture (PMUC), renal pelvis urine culture (RPUC) and renal stone culture (RSC). One hundred and twenty-two patients who underwent PCNL were enrolled. All patients were tested with PMUC: if negative they underwent a single-prophylactic dose of a third-generation cephalosporin during anesthetic induction; 4 patients (3.2%) had positive PMUC and received specific antibiotic treatment for at least 7 days prior to surgery or continued antibiotic treatment until a negative PMUC was obtained. Isolated agents were multidrug-susceptible E. Coli and S. Aureus. After surgery, patients were monitored for symptoms and signs of sepsis, which was confirmed with a new urine culture, two aerobic hemocultures and a thorax X-Ray to rule out pulmonary causes. Eighteen (14%) patients had a positive RPUC while seventeen (13,9%) had a positive RSC. Results from PMUC were different to those obtained from RPUC, which showed multidrug resistant bacteria and fungus. Considering this, they concluded standard recommended antibiotic prophylaxis would not cover these agents. Therefore, they recommend running RPUC and RSC, especially in patients at high risk of developing infectious complications to guide the eventual treatment. El-Agami et al. [18] conducted a prospective RCT comparing the rate of post-flexible ureteroscopy UTI in patients subjected to the standard antibiotic prophylaxis alone versus enhanced prophylactic measures. The study included 256 patients undergoing flexible ureteroscopy (FURS) for ureteral or renal stones. Patients in Group 1 received an intravenous injection of fluoroquinolone one hour before surgery, and oral antibiotics were used for 24 h postoperatively. Patients in Group 2 (enhanced prophylaxis) were tested with a urine culture ten days before the procedure; antibiotic-culture based was given for positive asymptomatic cases, while the procedure was deferred for active UTI. Postoperative, and overall complications were significantly higher in group 1 (15.6% vs. 6.3%, p = 0.04 and 26.6% vs. 17.2%, p = 0.047), respectively. Twenty patients (15.6%) in the standard prophylaxis group were diagnosed with UTI in comparison to 8 patients (6.3%) in the enhanced prophylaxis group (p = 0.047). Therefore, authors concluded that UTI after FURS could be reduced significantly by utilizing the suggested enhanced prophylactic approach.
Antibiotic prophylaxis vs. no prophylaxis in patients with sterile urine cultureLi et al. [19] conducted a prospective open-label RCT enrolling 109 patients undergoing RIRS. Patients were randomly assigned to one of three groups, receiving one of the following three treatments: a single dose of intravenous cefazolin (1 g), oral Cefuroxime (500 mg), and no prophylactic antibiotics. After surgery, no postoperative antibiotics were given unless febrile UTI was diagnosed. Febrile UTI was lower in the cefuroxime group (0%) than in the cefazolin group (9.4%, n = 3), but this difference was not statistically significant (p = 0.1). No statistical significance was found between the prophylaxis group and the no-prophylaxis group. In conclusion, as antibiotic prophylaxis could not reduce the incidence of postoperative febrile UTI and pyuria in patients with sterile urine undergoing RIRS, they suggested not giving antibiotic prophylaxis to this population to avoid antibiotic resistance and adverse events. Fourcade et al. [20] conducted an RCT to determine the importance of antibiotic prophylaxis before stone surgery (percutaneous or endoscopic) in patients with a preoperatory sterile urine culture. A total of 120 patients were divided into two groups: one received a single cefotaxime 1 g iv at induction of anesthesia, and the other received a placebo. Patient follow-up was divided into two periods: from day 1 to 3 and from day 3 to 30. The incidence of postoperative bacteriuria between the first and third postoperative days was significantly higher in the placebo group than in the cefotaxime-treated group (p = 0.014). The chemical stone type did not influence the outcome of postoperative infection. During the day 3 to day 30 follow-up period, no infection symptoms occurred in the cefotaxime group, while seven infectious episodes were noted in the placebo group (of which 6 UTIs). With an early postoperative infection rate of 23% in the placebo group as against 8.3% in the cefotaxime treated group (p = 0.014), this controlled study’s results favored antibiotic prophylaxis. The study by Hsieh et al. [21] aimed to determine the efficacy of prophylactic antibiotics in reducing post-surgical infections in patients undergoing URS. They conducted a double-blind, prospective, randomized controlled trial, enrolling 206 patients with preoperative sterile urine undergoing URSL. Patients were randomly allocated, in a ratio of 1:1:1:1, to receive prophylactic antibiotics with a single dose i.v. Cefazolin (1 g), Ceftriaxone (1 g), or oral Levofloxacin (500 mg), or no treatment (control group), respectively. Urinalysis and urine cultures were obtained between postoperative days 5 and 7. The rates of postoperative pyuria were significantly lower in patients with prophylaxis than in the control group (48.4 vs. 64.7%, P = 0.04). Patients receiving prophylaxis with levofloxacin and ceftriaxone had a significantly lower risk of pyuria than the control group (52.0 and 36.5 vs. 64.7%, respectively; P < 0.05). The rates of bacteriuria and fUTI tended to be lower in patients with prophylaxis, although the difference was not significant (4.5 vs. 11.8%, P = 0.09, 1.3 vs. 5.9%, P = 0.09). There was no significant difference in rates of bacteriuria and fUTI between the four groups. Patients with proximal stones had a higher risk of developing postoperative fUTI (odds ratio 9.35; P = 0.03). The authors concluded that antibiotic prophylaxis significantly reduces the incidence of pyuria after URSL and tends to diminish the risk of bacteriuria and UTI. Knopf et al. [22] conducted a study to determine whether perioperative single-shot prophylaxis in connection with a URS stone removal influences the rate of postoperative UTI. One hundred and thirteen patients were included in this prospective randomized study. In 57 patients, 250 mg Levofloxacin p.o. was given approximately 60 min before ureteroscopy, and 56 patients had no prophylaxis. In the group without prophylaxis, the rate of postoperative significant bacteriuria was significantly higher than in the group with prophylaxis (seven patients [12.5%] vs. one patient [1.8%]) (p = 0.026). In six cases, there was an E. coli bacteriuria. Additionally, a K. Pneumoniae and a non-specified Staphylococcus bacteriuria were detected in other cases. In conclusion, the authors suggest a single-shot prophylaxis using 250 mg Levofloxacin p.o. can be considered a valuable prophylaxis option. In addition, perioperative single-shot prophylaxis may be beneficial in case of an unexpected intraoperative complication, e.g., ureter perforations.
Antibiotic prophylaxis: fosfomycin tromethamine vs. standard of careThe primary endpoint of Qiao et al. [30] prospective, multicenter, RCT was to define the incidence of infectious complications (defined as asymptomatic and symptomatic bacteriuria, fever, urosepsis, bacteremia, and genitourinary infection) in patients undergoing RIRS. They enrolled 2016 patients and randomly divided them into two groups: the first received fosfomycin tromethamine, while the control groups received antibiotics according to local standard of practice (second-generation cephalosporin, fluoroquinolones, and other intravenous antibiotics). The overall incidence of infections following lithotripsy was 4.6%, with no statistically significant difference between study groups. Authors concluded fosfomycin is a valid cost-effective alternative to cephalosporin and fluoroquinolones for prophylactic purposes. Gokalp et al. [24] conducted a non-randomized controlled study enrolling 186 patients undergoing RIRS. Preoperative urine cultures were collected from all patients before surgery and, if positive, the intervention was postponed. Patients were divided into two groups: Group 1 (n = 49) received an oral dose of 3 g of Fosfomycin tromethamine administered 4–6 h before surgery; Group 2 received intravenous 1 g third-generation Cephalosporin (ceftriaxone) 30 min before surgery and an additional dose 6 h after surgery. The authors found no statistically relevant difference between the groups in terms of postoperative fever and UTI (p = 0.408 and p = 0.438, respectively) and suggested the use of Fosfomycin tromethamine as preoperative prophylaxis, even in patients with a positive preoperative urine culture.
Antibiotic prophylaxis: ciprofloxacin vs. cefotaximeOmar et al. [25] conducted a prospective study in patients with preoperatory sterile urine culture before PCNL. Between February and October 2016, 84 patients were enrolled. These patients were divided into two groups: 1°) 41 patients were given a single dose of 200 mg ciprofloxacin infusion, and 2°) 43 patients were given 2 mg of cefotaxime divided into two doses. Two (5%) patients in the ciprofloxacin group developed fever compared to 12 (28%) patients in the cefotaxime group. Twelve patients in the ciprofloxacin group (29%) and 14 in the cefotaxime group (33%) had a positive stone culture. RPCU was positive in 7 patients in the ciprofloxacin group and 10 patients in the cefotaxime group (17% vs. 23%). None developed clinical septic shock. In the ciprofloxacin and cefotaxime groups, SIRS 4% vs. 7% and fever 1% vs. 5% were identified, respectively. A prophylactic regimen consisting of a single dose of ciprofloxacin infusion during surgery induction showed a higher efficacy as a preoperative antibacterial preparation. Korets et al. [26] conducted a prospective study to define the correlation between the development of SIRS and preoperative UC, intraoperative RPUC and SC in patients undergoing PCNL. From February 2009 to February 2011, 198 patients were enrolled. All patients with a negative UC received a preoperative dose of prophylactic intravenous broad-spectrum antibiotics, which were continued for 24 h postoperatively. If the UC was positive, it received a minimum 7-day course of oral antibiotics based on the sensitivity profile. Broad-spectrum intravenous antibiotics were used at induction. At induction was administered broad-spectrum intravenous antibiotics. UC was positive in 47 cases (23.5%); RPUC in 21 (10.3%); SC in 33 (16.2%). SIRS was noted in 20 cases (9.8%); 6 of the 20 patients (30%) required intensive care treatment. Compared to patients without a postoperative-SIRS, those with SIRS were more commonly female (75% vs. 46%), had longer operative time (146 min vs. 113 min), had a higher rate of positive pelvic (26% vs. 10%) and stones (44% vs. 17%) cultures. Even appropriate treatment of preoperative urinary infections may not prevent a postoperative systemic response after PNL but it seems to result in a decreased rate of bacteremia and possibly hastened recovery from SIRS. Kobayashi et al. [27] aim to study the influence of preoperative antimicrobial treatment on intraoperative culture (IC) results and infectious complications in patients with positive preoperative bladder urine culture (PBUC) undergoing ureteroscopic lithotripsy. They enrolled 162 patients from April 2019 to March 2020. Based on PBUC findings, they were divided into positive and negative PBUC groups. Preoperative antimicrobial treatment was administered to the positive PBUC group while the negative PBUC group received perioperative antimicrobial prophylaxis only. IC, including bladder urine culture, renal pelvic urine culture, and stone culture, were collected. In the positive PBUC group, 19 (28.4%) patients had positive bladder urine cultures after the antibiotic treatment. Positive ICs (43.3% vs. 3.2%, p < 0.001) and post-operative fever (16.4% vs. 2.0%, p = 0.001) were more common in the positive PBUC group than in the negative PBUC group. In the positive PBUC group, 11 patients had a postoperative fever, regardless of the ICs results (6 positive ICs and 5 negative ICs). Furthermore, antimicrobial-resistant bacteria were detected from ICs in 5 patients with positive PBUC, including 4 suffering from a post-operative fever. Although the effect of pre-operative antimicrobial treatment is not definitive, to avoid serious infectious complications, authors concluded that careful infection control, based on the pre- and intra-operative culture results, should be performed at least in high-risk patients. Mariappan et al. [28] conducted a prospective study to evaluate whether 1 week of ciprofloxacin before surgery reduces SIRS in patients with stones > 2 cm or with pelvi-calyceal dilatation undergoing PNL. All the 98 patients included had negative urine culture before PNL. All patients received iv gentamycin 5 mg/kg at induction. In the ciprofloxacin-treated group there was a significant reduction of SIRS (7% vs. 18%) with an incidence three times less of infected pelvic urine. Song et al. [29] conducted a prospective study to evaluate the antibacterial effect of Fosfomycin tromethamine (FT) on the bacteria inside urinary infection stones in patients undergoing PNL. A total of 112 patients with a negative urine culture were examined from May to December 2018. The patients were divided into two groups: the experimental group received oral FT 3 g/day, and the control group received intravenous infusion of cefuroxime 3 g/day. The measured drug concentrations inside the stones suggest that the drug concentration within the stones in the experimental group was significantly higher than in the control group. The colony count in the stone cultures from the experimental group was also lower than the control group. There was no significant difference between the two groups in postoperative fever risk. Moreover, the SOFA scores showed that the risk of systemic organ failure was significantly lower in the experimental group (SOFA > 2 control group 33.26% vs. experimental group 10%).
Comments (0)