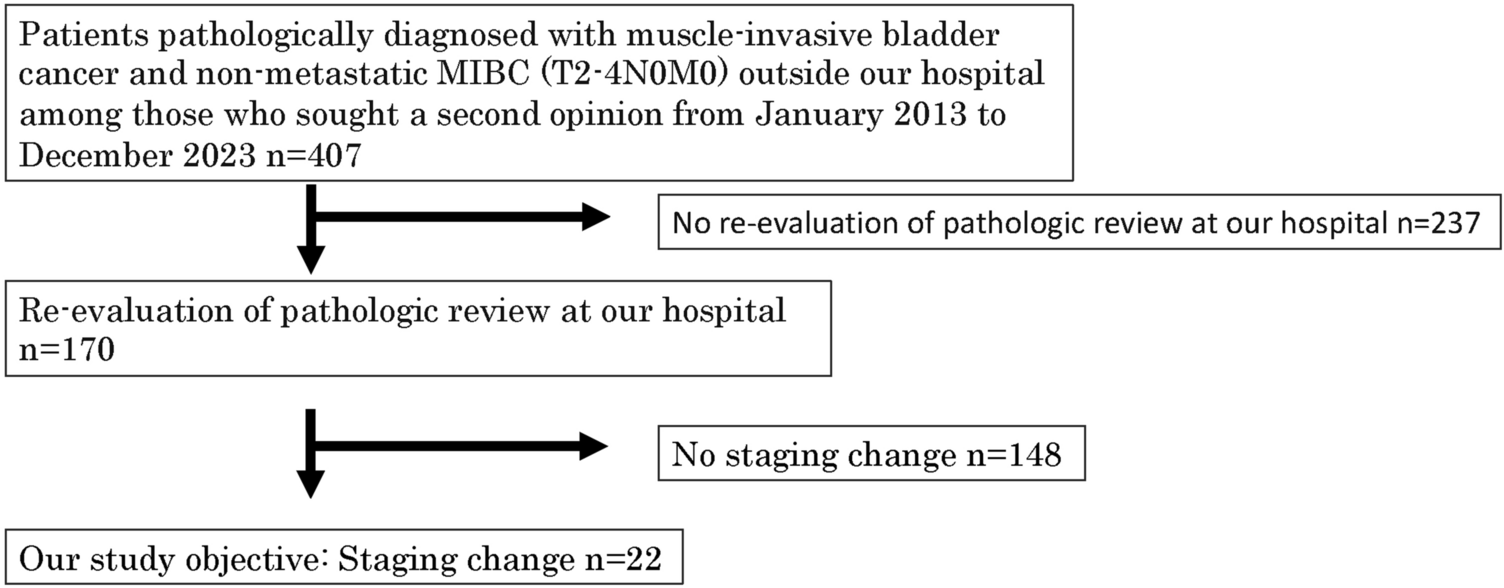
A retrospective cohort study was performed of patients who had been diagnosed with pelvic mesh in viscus and had undergone management at three tertiary urogynaecology centres. Ethics committee approval was obtained from Greenslopes Research and Ethics Committee (Protocol 18/62 GPH), Gold Coast Health Human Research Ethics Committee (HREC/2019/QGC/52891) and Metro South Human Research Ethics Committee (HREC/2023/QMS/94812). Patients who had undergone management of mesh in viscus from April 2007 to April 2023 were identified from hospital records. Paper and electronic hospital records were reviewed. Data was collected on patient demographics, mesh type and details of original surgery, presenting symptoms, prior treatments in other centres, investigations, management and surgical/post-operative outcomes and symptoms. All patients who had been diagnosed with mesh erosion into viscus were eligible for inclusion.
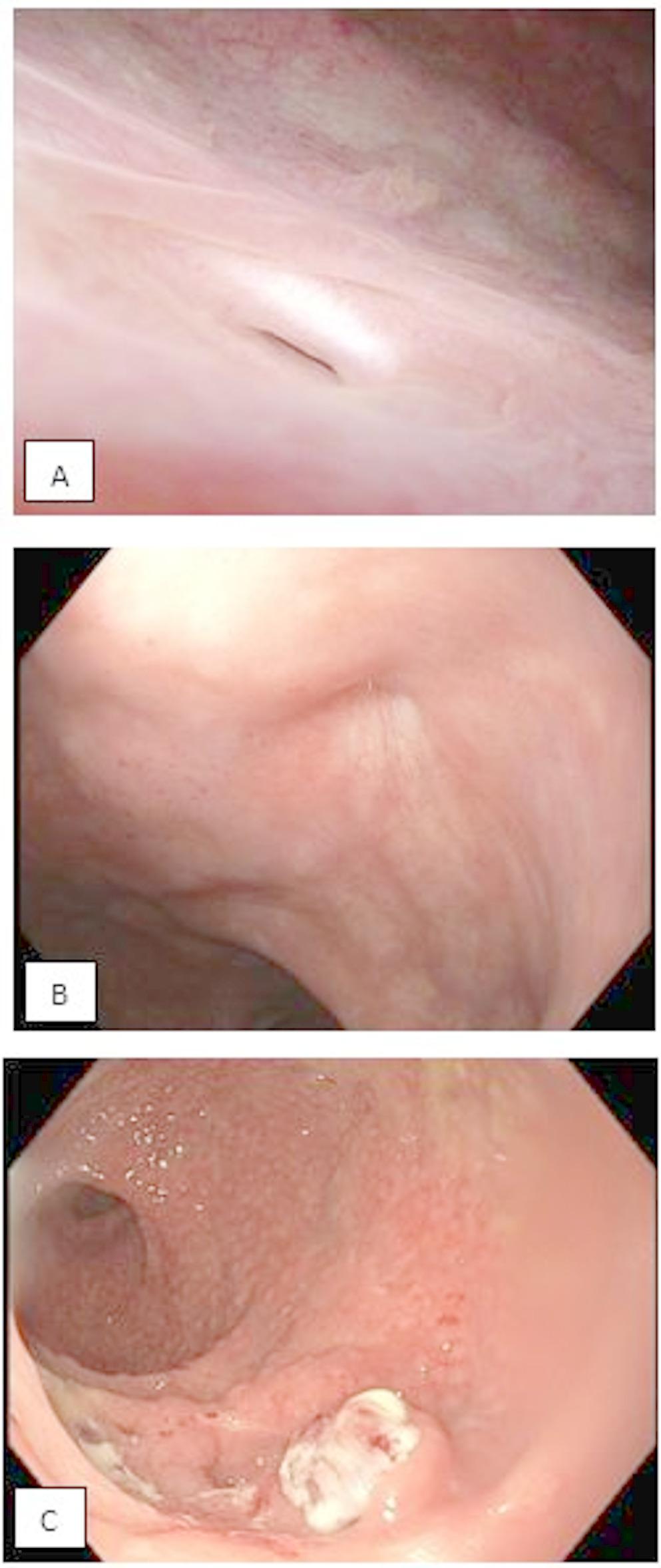
All patients underwent standardised history-taking and clinical examination. Medical records of previous mesh implantation surgery were obtained. All patients underwent standardised examination of vagina/rectum and cystourethroscopy for diagnosis, performed under general anaesthesia (GA) or sedation. Cystourethroscopy involved use of a 70-degree, 30-degree and/or a 0-degree cystoscope. The bladder was distended to maximum capacity, to exclude mesh perforation not apparent at lower volumes and other pathology.
If there was suspicion of genitourinary fistula, a methylene-blue dye test was performed. This involved instilling at least 200 ml dilute methylene-blue dye into the bladder via Foley catheter, while observing for vaginal leak with aid of a speculum. If there was possible rectovaginal fistula, betadine solution was instilled per rectum via Toomey syringe to assess for vaginal leak.
All patients were counselled regarding their options including conservative or minimally invasive management, partial excision of mesh involved and viscus repair, and complete excision of the mesh involved and viscus repair.
Partial excision of slings or TVM involved vaginal incisions. Complete excision of implants involved vaginal and groin incisions for trans-obturator slings and TVM; vaginal and small Pfannenstiel incision for retropubic slings and sacrocolpopexy mesh.
Repair of bladder
Surgical repair of bladder was undertaken transvaginally or transabdominally depending on the location of mesh erosion. Ureteric catheterisation was performed if mesh erosion was close to the ureteric orifices. Following excision of bladder mesh, the extent of the bladder defect was identified, and the bladder dissected from surrounding vagina to allow tension-free repair. The bladder was repaired in two layers with absorbable sutures (2–0 polyglactin). Following this, a methylene-blue dye test was performed to confirm a watertight closure. The Foley catheter was left in situ for two weeks with oral antibiotic cover, followed by an outpatient methylene-blue dye test to exclude fistula and an immediate trial of void (TOV) if negative.
Repair of urethra
Surgical repair of the urethra was carried out transvaginally following transvaginal excision of urethral mesh erosion. Excision of urethral mesh was performed through the mesh perforation sites without additional urethrotomy. Dissection of the urethra from surrounding vaginal tissue was performed to allow tension-free repair. Closure of the urethral defect was performed in two layers with interrupted absorbable sutures (3.0 polyglactin), in a horizontal manner to reduce risk of urethral stricture.
A methylene-blue dye test was then performed to ensure watertightness. Following urethral repair, a labial fat flap or modified Martius flap was routinely performed. A Foley catheter was left in the bladder for 3 weeks, followed by an outpatient methylene-blue dye test to exclude fistula and TOV if negative.
With regards to our units’ technique for performing a labial fat flap, it has some similarities to that described by Wilson et al. [15]. The key differences include that our unit makes a smaller incision starting at a level lower than the mons pubis in order to avoid a large labial scar or labial distortion. Generally, suture ligation is not required as the flap is divided with diathermy. Strict haemostasis is observed and a drain is not routinely placed within the labial wound.
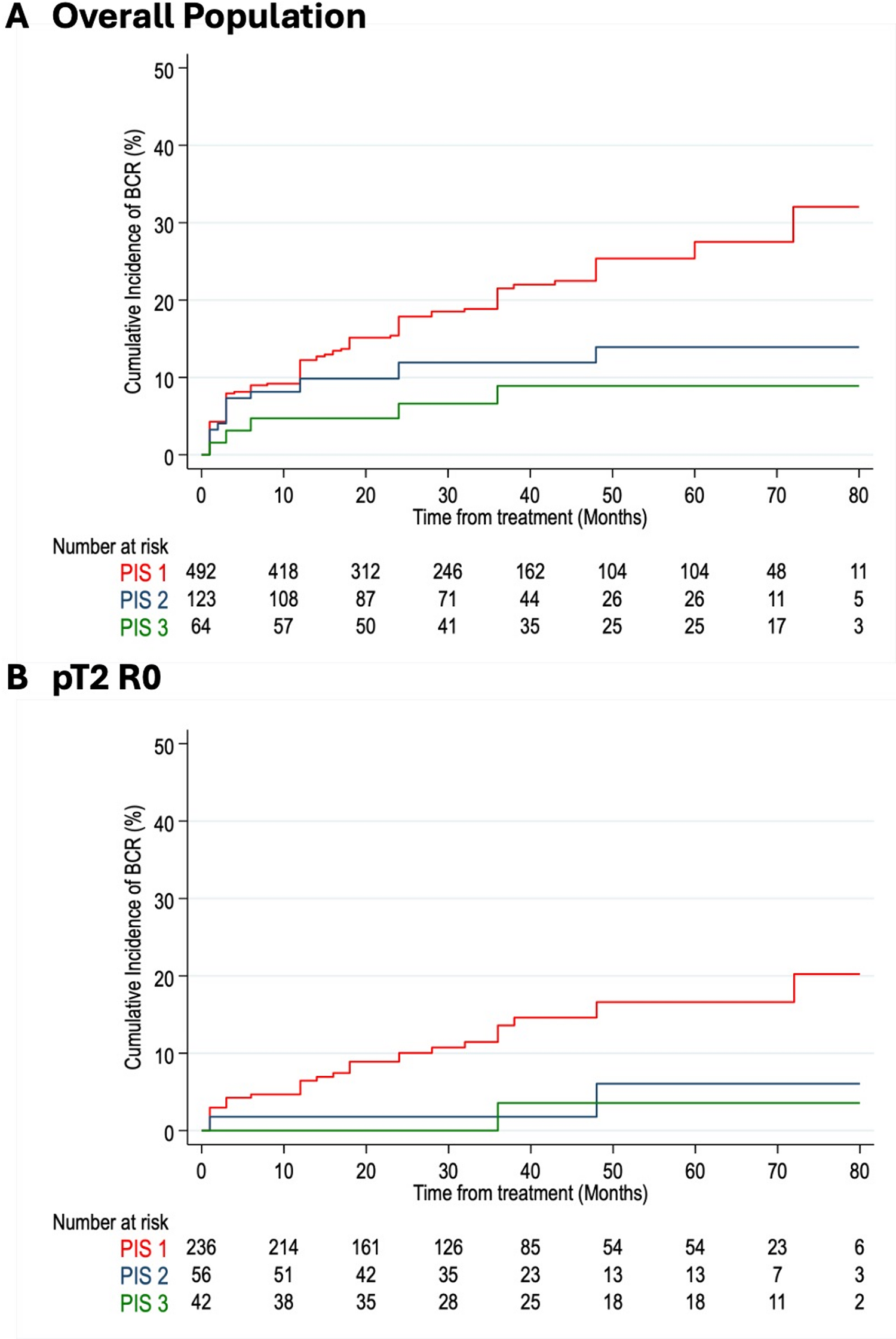
Primary outcome was successful viscus repair, as determined by a negative methylene-blue dye test at two to three weeks postoperatively. Secondary outcomes included resolution of presenting symptoms at 3 months including pain, UI and rUTIs. All patients were followed up at 6 weeks and 3 months post-operatively, and longer when clinically required. Data was analysed using Microsoft Excel and Stata version 18 (Stat, Statacorp LLC, Texas, USA). Statistical analysis of pre-operative and postoperative symptoms was performed using McNemar’s chi-square test. A p value < 0.05 was considered statistically significant.



Comments (0)