
Remember me
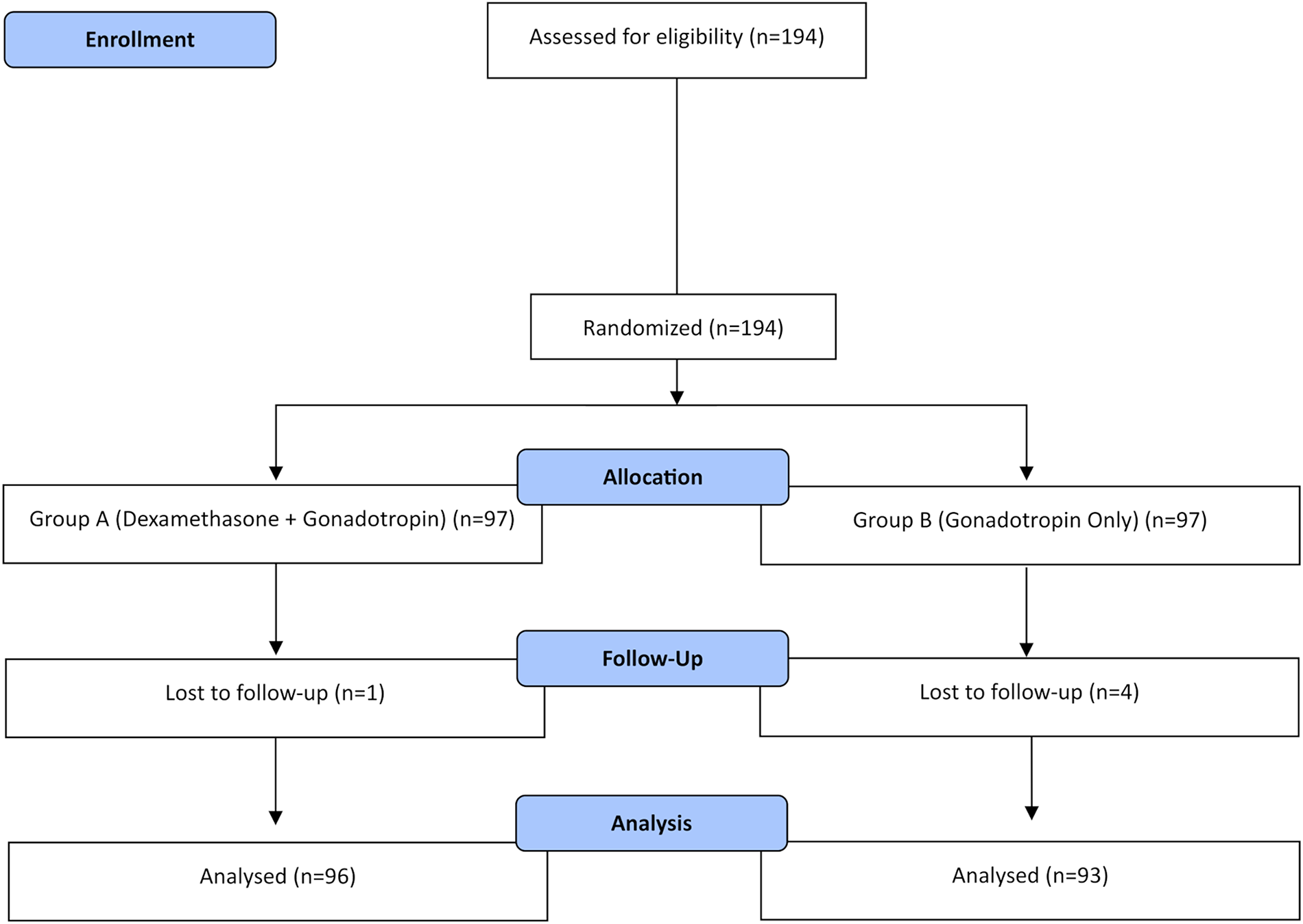

As shown in Fig. 1, this was a retrospective study conducted at the Reproductive Center of Nanjing Women and Children’s Healthcare Hospital from January 2018 to December 2022. 4172 blastocysts from 941 PGT-A cycles were incorporated, which were fertilized by ICSI and biopsied on day 5/6/7 with next generation sequencing (NGS). 538 blastocysts were selected to transfer according to their NGS results in the following single euploid FET cycles. Cycles were excluded if the embryos were from donor oocytes, biopsy results were inconclusive or involved women were diagnosed with uterine malformation.
Fig. 1
Flow chart of the retrospective cohort study
Ovarian Stimulation ProtocolAll participants underwent a gonadotropin-releasing hormone (GnRH) antagonist protocol to stimulate the ovarian. Briefly, recombinant follicular stimulating hormone (rFSH, Gonal-F, Merck Serono, Italy) was administrated, varying from 150 to 225 IU per day, on the third day of the menstrual period. The ovarian response and follicular growth were monitored by ultrasound scan and sex hormone levels (FSH, estradiol, luteinizing hormone, and progesterone). Moreover, the dose of gonadotropin (Gn) was adjusted to cause pituitary suppression. When the diameter of at least two dominant follicles reached 18 mm, a dose of 10000 IU human chorionic gonadotrophin (hCG, Lizhu, China) was injected to trigger the ovulation.
Oocyte Collection, ICSI and Embryo Culture36 h after hCG injection, vaginal oocyte retrieval was performed under the ultrasound guidance. Then, ICSI was used for all PGT-A cycles in our study, and was conducted 4–6 h after oocyte collection. The embryos were cultured to the blastocyst stage in Vitrolife sequential medium (Goteborg, Sweden) and a humidified atmosphere containing 5% O2 and 6% CO2 and 89% N2.
Blastocyst Grading, Biopsy and PGT-ABlastocyst evaluation was assessed based on its degree of expansion and the morphology of ICM and TE prior to embryo biopsy by two experienced embryologists. According to the criteria presented by Gardner and Schoolcraft [1], blastocyst expansion was classified into six grades: 1: the blastocele filling < 50% of blastocyst; 2: the blastocele filling > 50%; 3: a full blastocoele filling the blastocyst; 4: an expanded blastocyst with the thinning zona, the blastocoele volume larger than that of the full blastocyst; 5: a hatching blastocyst, the TE starting to herniate out of the zona; 6: a hatched blastocyst, the blastocyst completely escaping from the zona. The ICM was assigned one of the following three grades: A: numerous tightly packed cells; B: several and loosely packed cells; or C: very few cells. The TE was assigned one of the following three grades: A: many cells organized in epithelium; B: several cells organized in loose epithelium; or C: few large cells. In our center, the eligible blastocytes for biopsy were considered for expansion (4, 5, 6) and ICM or TE grade (AA, AB, AC, BA, BB, BC, CA and CB) on day 5, 6 or 7. TE biopsies were performed as previously described [20]. A laser (Hamilton Thorne Inc., Beverly, USA) was used to open the zona pellucida of blastocyte to allow the passage of biopsy pipette. The biopsy pipette was then pressed against the TE and gently aspirated 4–5 cells into the pipette. 2–3 laser pulses were performed at the junctions among cells and TE cells were separated. Samples were then tested and analyzed by a PGT company (Yikon, Beijing, China) with testing qualification. NGS on the sample of TE cells was conducted under the protocol described by Nagy et al. [21], mainly involving whole-genome amplification (WGA) with a SurePlex DNA Amplification System (Illumina, San Diego, CA, USA), sequencing for 24 chromosome aneuploidy screening with a VeriSeq PGT Kit (Illumina, San Diego, CA, USA) in line with the manufacturer’s recommendations. According to the screening results, blastocysts were diagnosed as euploid, aneuploid or mosaic.
Vitrification and Warming ProceduresEmbryo vitrification and warming followed the previous procedures [6]. After biopsy, blastocysts were firstly equilibrated in vitrification solution 1 (Kitazato BioPharma Co., Shizuoka, Japan) at room temperature for 12 min. Then, the embryos were transferred to vitrification solution 2 at room temperature for 1 min, placed on the tip of Cryotop (Kitazato BioPharma Co.) and put into liquid nitrogen. For thawing, the film strip of the Cryotop device containing the blastocyst was quickly submerged in 0.3 ml of warming thaw solution 1 (Kitazato BioPharma Co.) containing 1.0 M sucrose, at 37℃, for 1 min, followed by transfer of the blastocysts to the second thaw solution 2 containing 0.5 M sucrose and incubation for 3 min. Finally, blastocysts were washed in basic solution 3 and 4 at room temperature for 5 min, and then were transferred into 50 μl droplets of G2 medium (Vitrolife) under mineral oil. Assisted hatching were used before culturing in incubator according to the protocols previously described [22], and blastocysts were transferred after 2–4 h incubation.
Endometrial Preparation and Embryo TransferThe choice of endometrial preparation FET was based on clinical discretion and patient preferences. Women with regular menstruation usually underwent natural FET cycles in which follicular growth, endometrial thickness, and type were monitored from day 10 to 12 of their menstrual cycles, using serial transvaginal ultrasonography. When the dominant follicle was larger than 18 mm, the progesterone level ≤ 1.5 ng/ml, and the endometrial thickness ≥ 7 mm (as determined by tri-laminar lining), 10,000 IU hCG was injected. It took about 24–48 h after hCG administration to confirm the ovulation by ultrasound. 10 mg oral dydrogesterone (Abbott Biologicals B.V., Netherlands) was administered three times daily on the day after ovulation to support the luteal phase.
In artificial FET cycles, estradiol valerate (progynova, Bayer, France) was took 4–6 mg per day from the second day of the menstrual cycle for 1 week and adjusted to 8–10 mg on account of the endometrial thickness and serum estradiol (E2) level. This group was further divided according to the addition of GnRH agonist (triptorelin acetate, Diphereline, IPSEN, France), which was administered at the early part of the follicular phase (days 2–4) during the menstrual cycle. After downregulation was confirmed by baseline hormonal (E2 level > 30 pg/ml, luteinizing hormone and FSH levels < 5 IU/L) and transvaginal ultrasound assessment (endometrial thickness < 5 mm), daily 4–6 mg oral estrogen was commenced. When the endometrial thickness reached 7 mm and serum E2 level peaked at 200 pg/ml, 90 mg vaginal progesterone (Crinone, Merck Serono, UK) once a day and 10 mg dydrogesterone three times daily were administered.
It took 6–7 days for embryo transferring after hCG trigger in natural FET cycles and 5 days after progesterone supplementation in artificial FET cycles. One frozen euploid embryo was picked out at a time, based on morphological score and thawed for transferring.
Outcome MeasuresPrimary outcomes were euploidy and live birth rates. Euploidy rate was calculated as the number of euploid embryos with 46 chromosomes divided by the total number of biopsied embryos with genetic results. Furthermore, euploidy rate was compared for different blastocyst morphology (expansion, ICM and TE grades) and developmental rate (Day 5, 6 and 7). The primary endpoint was live birth rate after single euploid FET. The live birth rate was defined as the number of live births divided by the sum of embryo transfer cycles included in the cohort. Live birth was considered when a living fetus was born after 28 weeks of pregnancy.
Statistical AnalysisAll data analyses were performed using Stata 9.2 statistical software package (Stata Corp, LP). T test was used to compare the continuous variables; if the variances were far from equal, the Wilcoxon signed rank test was used on maternal age, maternal BMI, duration of infertility, basal FSH, LH, E2 and endometrial thickness. The chi-squared test was used to compare the categorical variables, such as type of infertility, indication for PGT-A and endometrium preparation. Multivariate logistic regression analysis was conducted to confirm whether embryo developmental rate and morphological parameters were independently related to euploidy rate and live birth rate after adjusting for confounding factors. The adjusted variables in the logistic regression model were those with a significance on univariate analysis at P < 0.05 or those that could potentially affect euploidy rate and live birth rate, including maternal age, maternal BMI, type of infertility, duration of infertility, indication for PGT-A, endometrium preparation, endometrial thickness, blastocyst developmental rate, expansion, ICM and TE). Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated for euploidy rate and live birth rate in relation to morphology parameters of blastocysts (Expansion, ICM and TE) and developmental rate by multivariate logistic regression analysis. All significance tests were two-tailed, and P < 0.05 was considered to be statistically significant.
Comments (0)