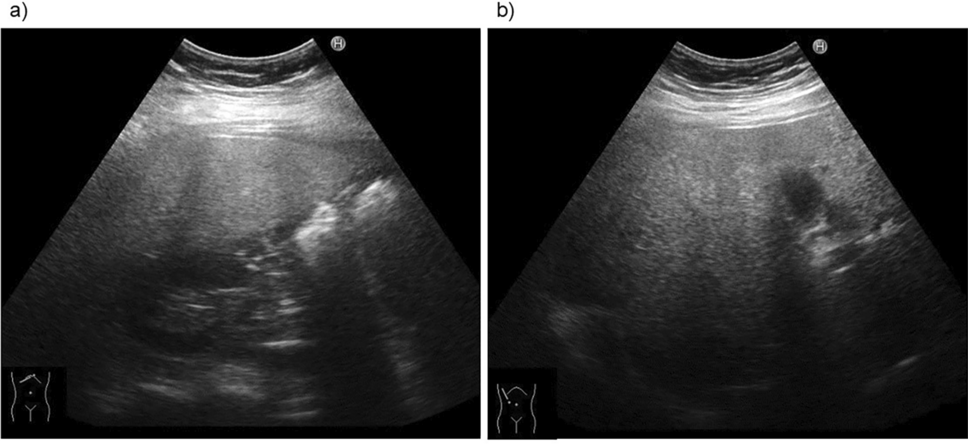
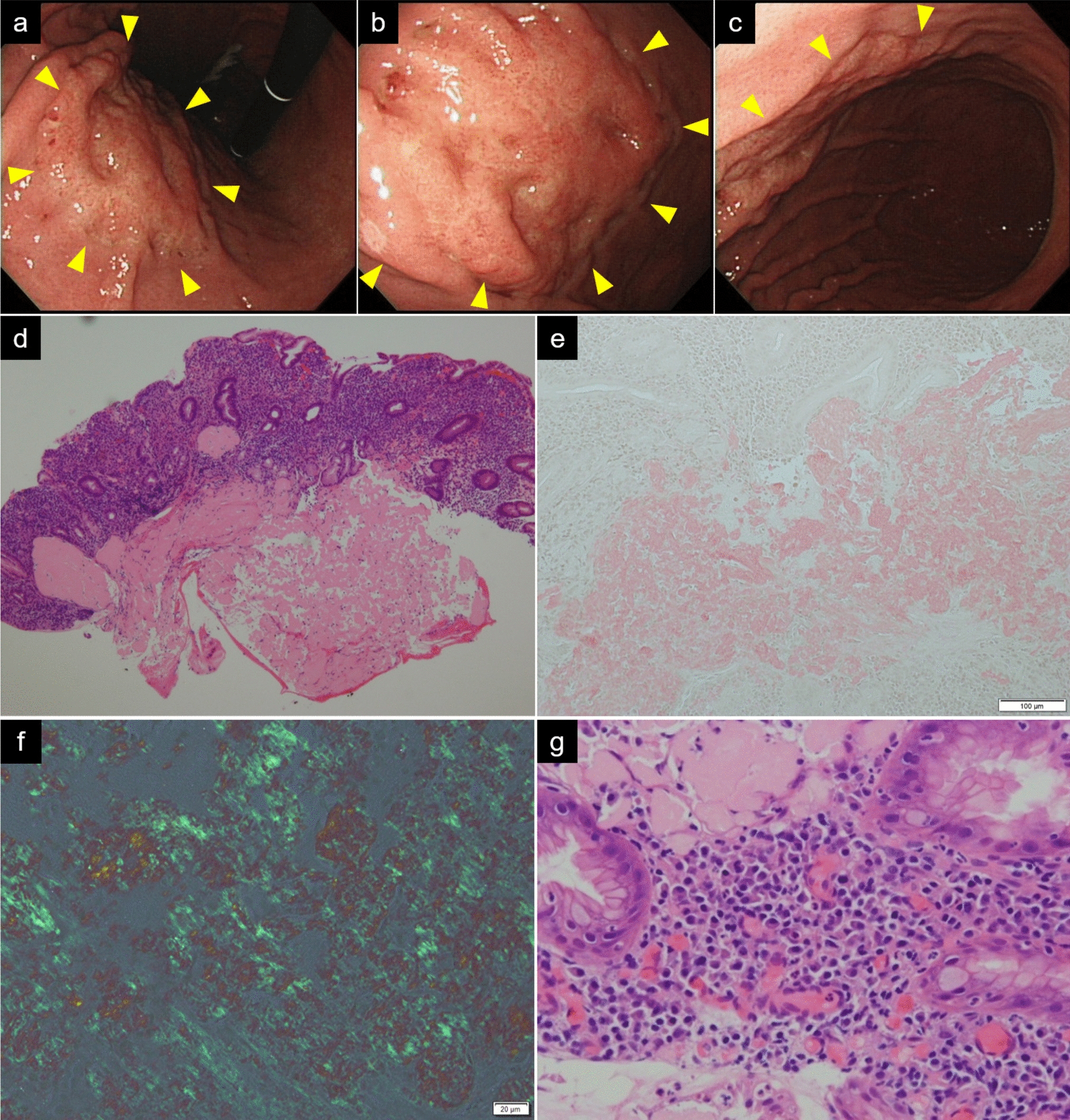
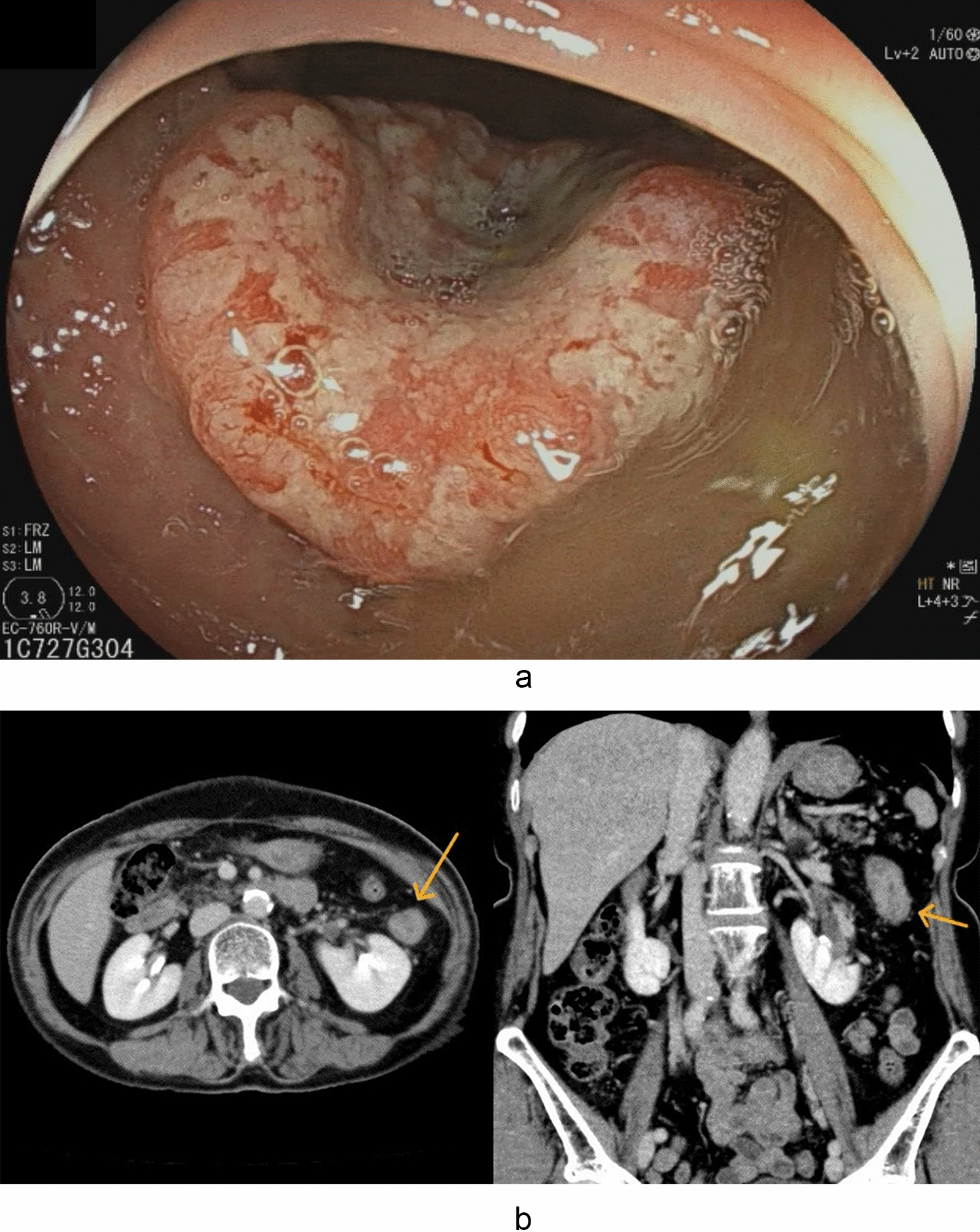
The disease extent of UC is usually confined to the colon and the rectum. However, the involvement of the upper GI tract has been recently reported [1, 5,6,7,8,9,10,11]. UC-associated upper GI lesions are characterized by diffuse inflammatory lesions in the stomach, duodenum, and/or intestine that resemble colonic lesions of UC on the basis of both endoscopic and pathological findings. In the present case, we suspected upper GI lesions because of the presence of epigastric pain and nausea, which are not usually seen as UC symptoms. The endoscopic and pathologic findings of the stomach and duodenum in our case are closely similar to the colorectal lesions of UC and consistent with UC-associated upper GI lesions. In the diagnosis of UC-associated upper GI lesions, other diseases, such as infectious disease and systemic vasculitis, must be excluded [8, 12, 13]. In the present case, CMV infection was ruled out according to the negative histopathology specimen and negative blood CMV antigenemia. Systemic IgA vasculitis was also ruled out because of the absence of systemic symptoms such as purpura, arthralgia, and renal involvement. Small bowel inflammation caused by COVID-19 is also an important consideration in the differential diagnosis. The CT scan of this patient showed no wall thickening in the jejunum and ileum, in contrast to the marked thickening observed in the duodenum and large intestine. Therefore, endoscopic examination of the small intestine distal to the duodenum was not performed. The colorectal lesions exhibited typical relapsing UC features, while the gastroduodenal lesions demonstrated UC-like endoscopic and histopathologic findings. Given these observations, we concluded that enteritis related to COVID-19 was deemed unlikely, and the diagnosis was consistent with upper GI involvement of UC.
While the treatment strategy for UC-associated upper GI lesions remains poorly established, these lesions are empirically known to improve by treatment for UC. Similar to treatment for colitis in UC, 5-aminosalicylic acid, corticosteroid, and anti-TNF alfa antibody can be used for UC-associated upper GI lesions or enteritis [7, 12,13,14,15,16,17]. In the present case, the good response to steroid treatment strongly supports that these lesions are UC-associated upper GI lesions. In this case, adalimumab was initiated following corticosteroid treatment. There were two primary reasons for selecting anti-TNF-α therapy. First, the patient had a history of 5-ASA allergy, which limited the available options for effective maintenance therapy. In the absence of 5-ASA treatment, the patient was considered at high risk for relapse. Therefore, we opted for an anti-TNF-α agent to ensure sustained remission. Second, anti-TNF-α antibodies are an appropriate treatment for active UC complicated by COVID-19 infection and are not considered a significant risk factor requiring special precautions. According to recent evidence, Nakase et al. analyzed Japanese IBD patients with COVID-19 and reported that immunosuppressive therapies other than corticosteroids (including thiopurines and anti-TNF-α agents) are associated with a relatively low risk of severe COVID-19 infection [18]. Furthermore, the British Society of Gastroenterology (BSG) guidelines recommend the combination of corticosteroids and infliximab for patients with severe UC during COVID-19 infection [19]. Based on these findings, we determined that anti-TNF-α antibody therapy would be appropriate for managing COVID-19-induced UC relapse. In the present case, the introduction of adalimumab proved to be an effective therapeutic strategy, as it did not exacerbate COVID-19 infection and successfully induced and maintained remission of UC with upper GI involvement.
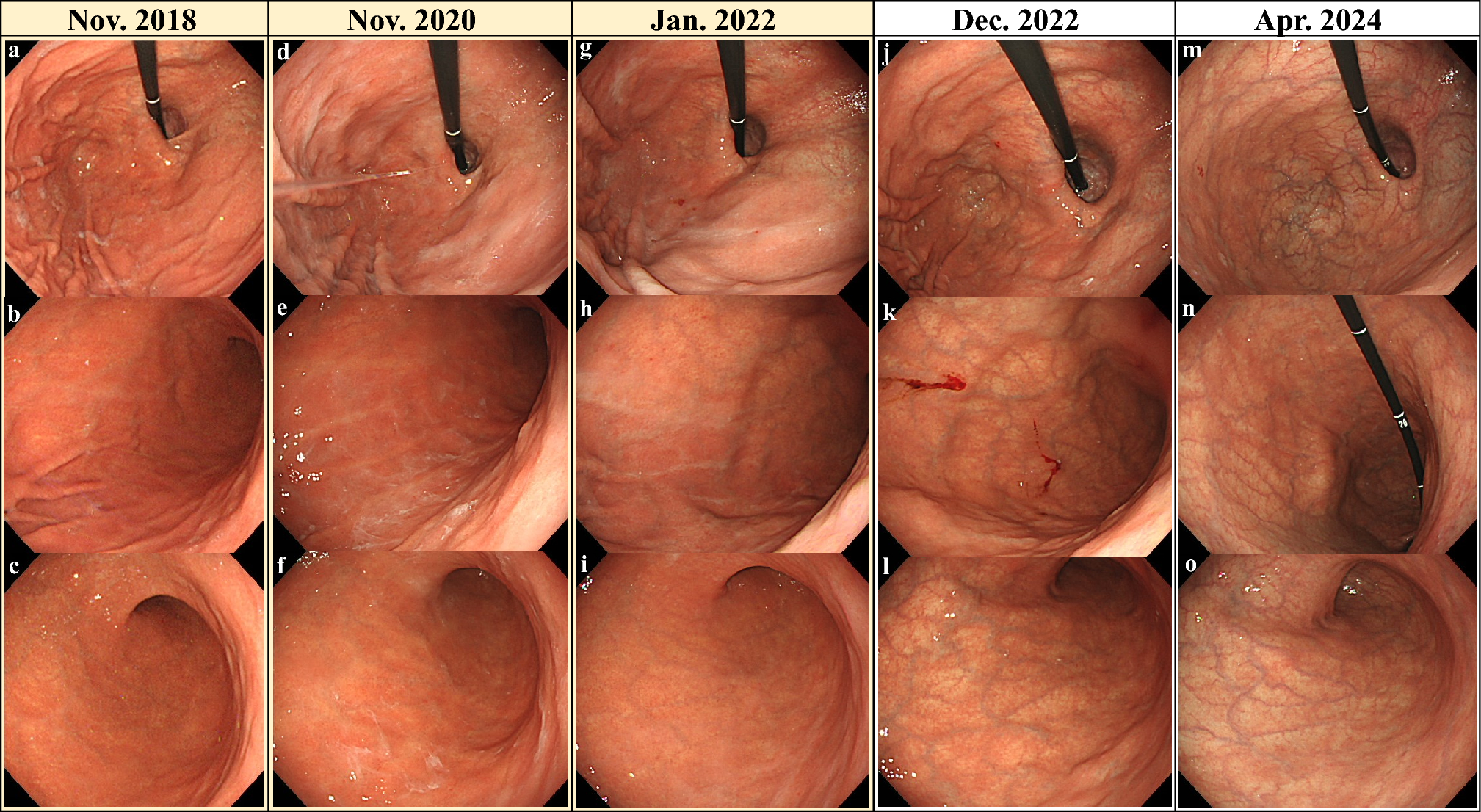
The triggers of upper GI inflammation in UC are still unclear. Most of the reported cases of UC-associated GI lesions were accompanied by pan-colonic UC, indicating that pan-colonic inflammation is strongly associated with upper GI inflammation [5, 6, 10]. A lower dose of prednisolone has been also reported as a possible risk factor for developing UC-associated upper GI lesions [5]. In addition, total or subtotal colectomy is one of the important triggers for the development of UC-associated upper GI lesions and small bowel lesions [8, 9, 11, 20]. Kohyama et al. reported that 42 (0.8%) out of 5284 UC cases had been diagnosed with UC-related postoperative enteritis [9]. However, the other triggers of UC-associated upper GI lesions remain largely unknown. The total colitis observed in our patient is similar to that seen in previously reported cases. Of note, in our case, the relapse of UC and the appearance of upper GI lesions occurred almost concurrently, immediately after COVID-19. A recent European cohort study has reported that COVID-19 has a slight impact on the course of inflammatory bowel disease (IBD) [21]. However, a multicenter study from Japan has described that COVID-19 changed the course of IBD in approximately 10% of patients [22]. Furthermore, the onset of UC triggered by COVID-19 has been reported in some patients [2,3,4]. Although evidence is still limited, these reports suggest that COVID-19 amplifies UC or causes UC by revealing masked inflammation. In the present case, UC relapsed approximately 7 days after the COVID-19 onset, despite being in remission for 3 years. The patient also developed UC-associated gastroduodenal lesions almost at the same time as the UC recurrence. Thus, the activation of the systemic immune system by COVID-19 may have caused the recurrence of UC and the development of UC-related upper GI lesions.
In conclusion, this report describes for the first time a rare case of relapsed pan-colonic UC accompanied by UC-associated GI lesions immediately after contracting COVID-19. COVID-19 can be a possible trigger of UC-associated upper GI lesion. In patients with UC infected with COVID-19, we should be aware of the development of upper GI lesions and the relapse or worsening of UC. Further studies are needed to understand the relationship between UC or UC-associated upper GI lesion onset and COVID-19.



Comments (0)