We presented a case with FMF and sigmoid colon stricture. The improvement of the sigmoid colon stricture following colchicine administration was remarkable. This case may yield valuable insights for identifying patients with FMF among those with CD.
FMF is an inherited disease diagnosed according to the Tel-Hashomer criteria, and it is believed that there are more than 100,000 patients with FMF worldwide [7]. According to this criterion, FMF is divided into two types, “typical” and “atypical,” on the basis of clinical findings. Fever, abdominal pain, chest pain, and frequently joint pain and rash due to peritonitis are the main symptoms of FMF [1], and the differential diagnosis between FMF and CD is very challenging owing to the highly similar clinical presentations.
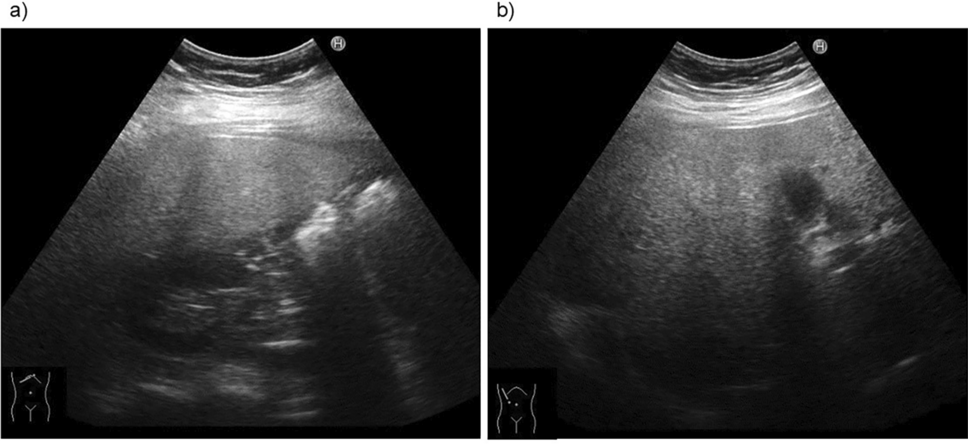
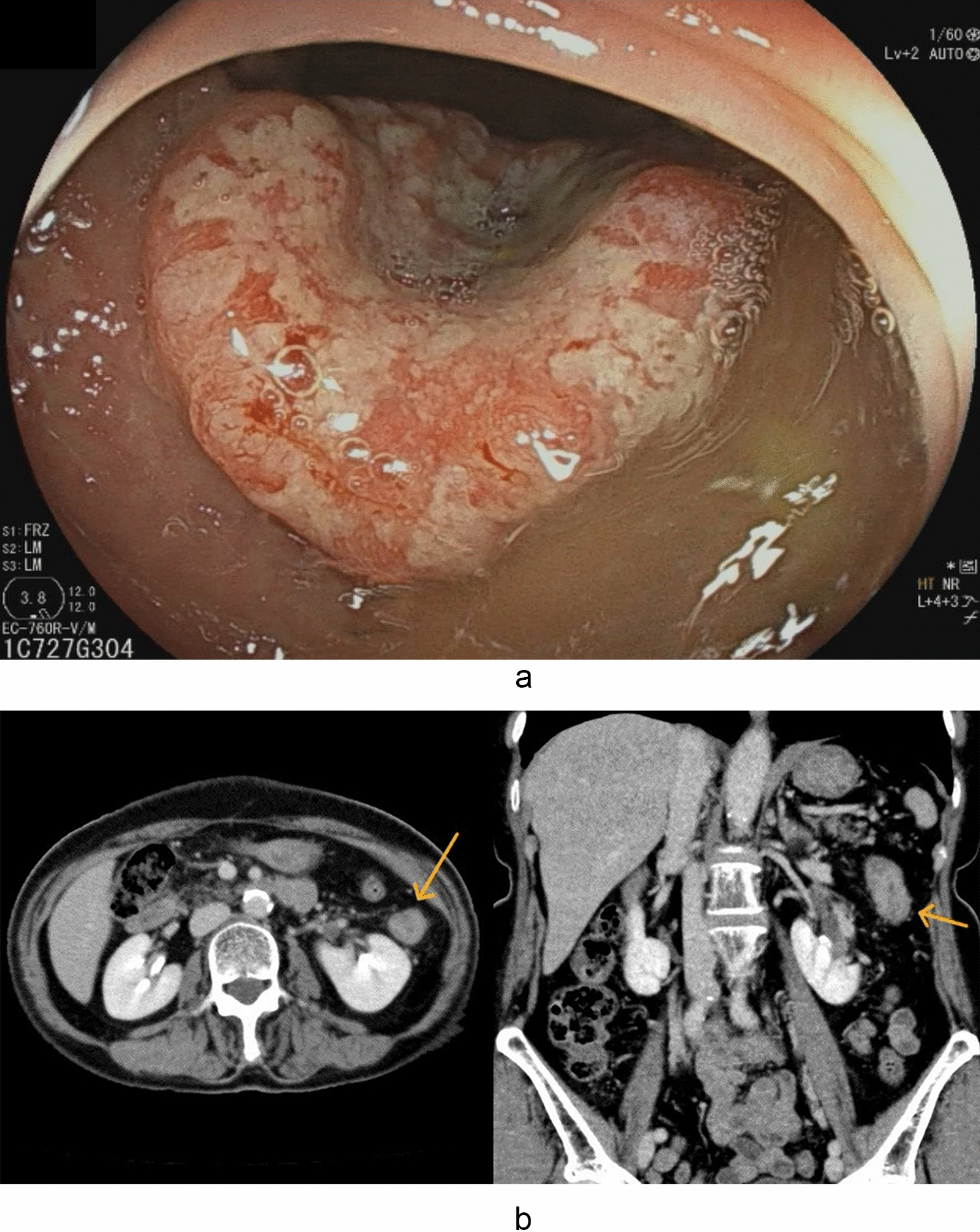
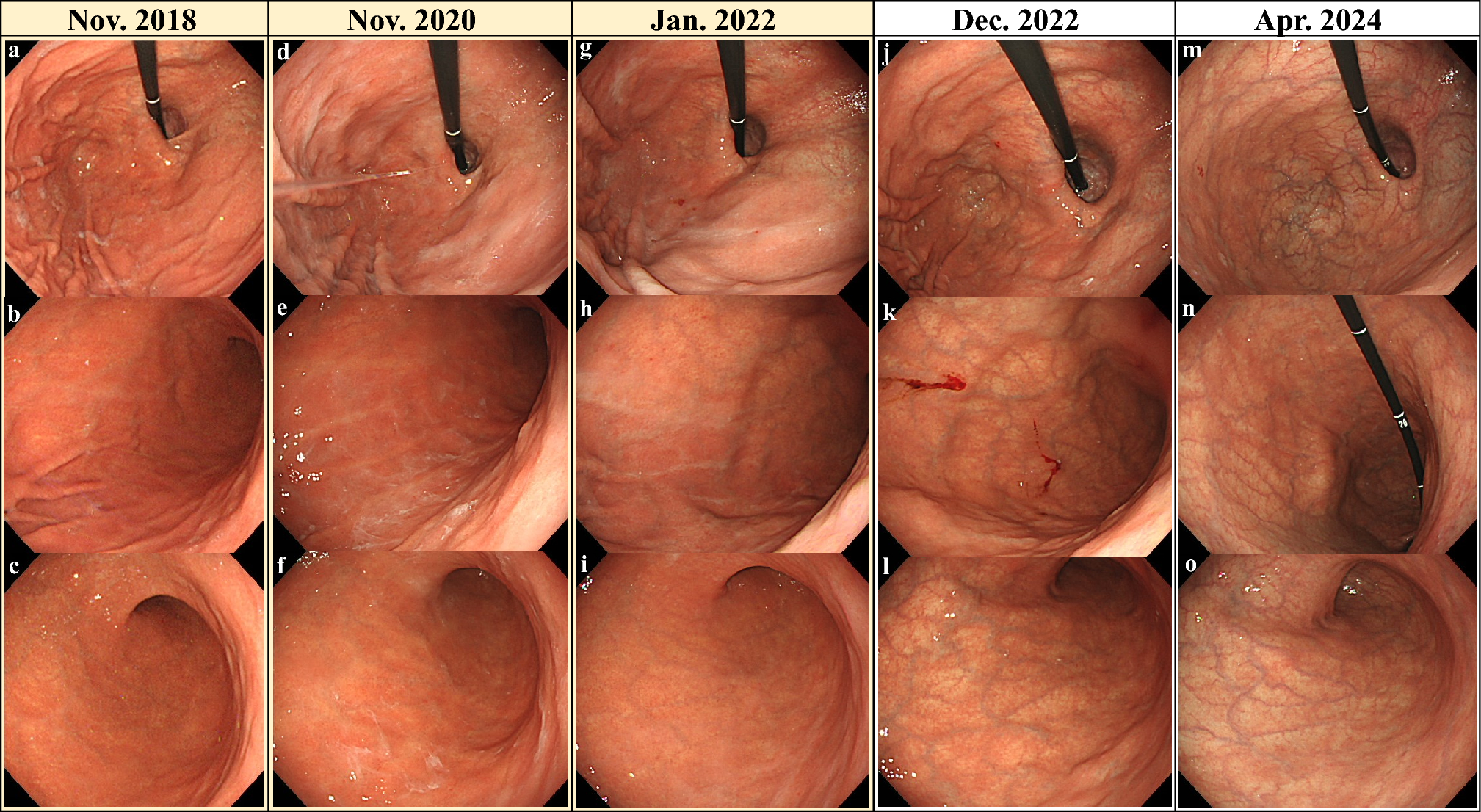
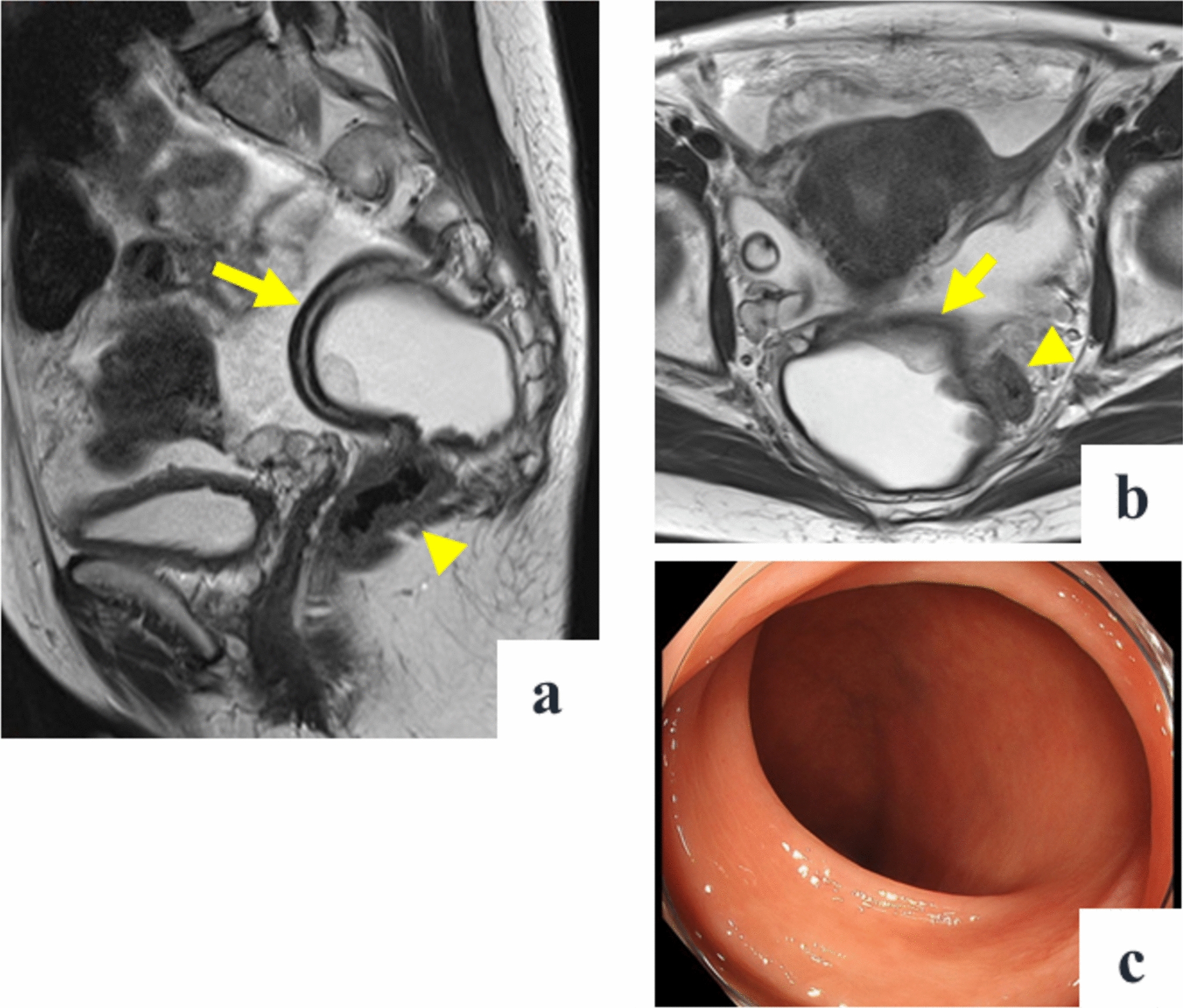
Here, FMF was suspected owing to repeated episodes of fever and abdominal pain lasting for several days monthly; however, the patient was initially diagnosed with CD with sigmoid colon stricture. During the episodes, CRP and SAA levels markedly increased, and CT and intestinal ultrasonography revealed extensive wall thickening of the small intestine and sigmoid colon. Furthermore, muscular defense and rebound pain due to peritonitis were confirmed, and the patient was diagnosed as a typical case of FMF. Colchicine was highly effective, and after visiting our hospital, the patient’s fever and abdominal pain disappeared for more than 2 years. Moreover, the bloody stools improved, and the sigmoid colon ulcer that hindered the passage of the colonoscope disappeared, thereby enabling the colonoscope to pass through.
In FMF, the function of pyrin, which activates inflammasomes and promotes caspase-1, IL-1β, and IL-18 production, is impaired owing to MEFV gene mutations, thereby resulting in inflammation. Pyrin plays a role in the permeability of the gastrointestinal mucosa, which is believed to contribute to gastrointestinal lesion formation [8]. The MEFV gene comprises 10 exons, and mutations in exon 10 of the MEFV gene, including M694V, V726A, and M694I, are common in patients with FMF in the Mediterranean region [9]. Conversely, mutations, including M694I, E148Q, L110P/E148Q, and P369S/R408Q, are more common in Japan [2]. Dimitri et al. argued that the E148Q mutation was a benign polymorphism because the frequency of the mutation was the same in patients with FMF and asymptomatic relatives [10]. Separately, it was reported that patients with the E148Q mutation showed the typical FMF phenotype [2]. Heterozygosity for the E148Q and L110P mutations was observed in the present case who showed typical FMF symptoms.
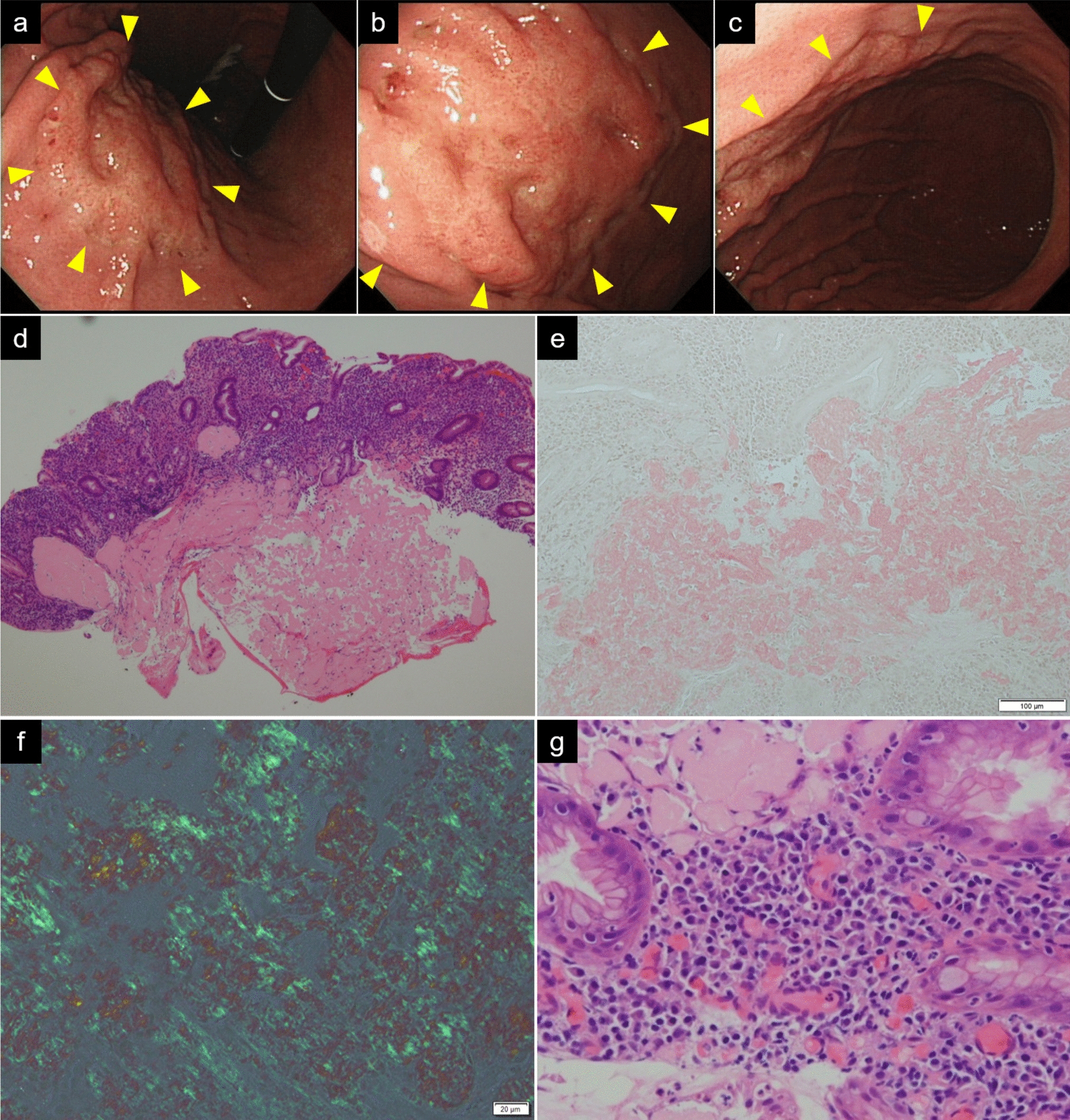
Several reports on endoscopic findings in FMF have been noted; however, no specific and consistent mucosal findings have been identified. Arasawa et al. reported pseudopolypoid-like lesions in the transverse colon [6], and Yokoyama et al. reported longitudinal ulcers in the terminal ileum and erythema, erosions, and ulcers in the ascending colon [11]. A study on the colonoscopy findings of eight cases of IBD unclassified (IBDU) with MEFV gene mutations revealed various mucosal lesions, rectal sparing, right-sided dominant colitis, pseudopolyposis, and granular protrusions [12]. Ezaki et al. reported a case of MEFV gene mutation-associated duodenojejunal pseudopolyposis [13]. Demir et al. reported 41 cases of FMF in which small-bowel lesions were diagnosed using capsule endoscopy and detected several erosions and ulcers in the jejunum [14]. Shibata et al. observed discontinuous loss of vascular markings, erosions, and friable mucosa, similar to ulcerative colitis, except in the rectum [15]. From these reports, the endoscopic findings of FMF may be analogous to those of IBD, and distinguishing between these diseases on the basis of endoscopic findings is difficult. This case showed a sigmoid colon stricture with longitudinal ulceration resembling CD. We considered performing small intestine examinations; however, even though the sigmoid colon stricture had improved, we considered it too narrow to perform a transanal balloon-assisted endoscopy. Moreover, the patient did not request a transoral balloon-assisted endoscopy or small-bowel capsule endoscopy as her symptoms had calmed down. Intestinal ultrasonography was performed during the critical phase, and although increased blood flow was observed on the serous side of the jejunum, no color Doppler signals were noted in the intestinal wall. No reports on the findings of intestinal ultrasonography in FMF are available; however, as increased blood flow in all layers was observed in the active phase of CD [16], it was suggested that increased blood flow on the serosal side can be useful in diagnosing FMF.
Regarding histologic findings, Agin et al. reported that 31% of patients with FMF who underwent colonoscopy had histologic findings suggestive of IBD, including goblet cell depletion, cryptitis, and crypt hyperplasia in the colon and terminal ileum [17]. In this case, noncaseating granulomatous cells were not detected; however, we confirmed the presence of cryptitis and diffuse inflammatory cell infiltration as observed in IBD. Therefore, as the histopathological differences between FMF and IBD have not been clearly elucidated, further research is warranted.
In this case, although FMF alone was the probable cause, the possibility that it was caused by a combination of FMF and CD cannot be excluded owing to prior endoscopic evidence of sigmoid colon narrowing. Twenty-five of 69 Armenian patients with IBD had FMF [18]. In a recent retrospective cohort study in Japan, MEFV mutations were detected in 238 of the 396 patients diagnosed with IBDU, with exon 2 mutations being the most common. Of the 134 cases, except for those with insufficient information on the clinical background and colchicine responsiveness, typical FMF and atypical FMF were 58 and 59 cases, respectively [19]. Gucenmez et al. reported that patients with FMF had significantly higher fecal calprotectin levels than those of healthy controls, suggesting that patients with FMF have asymptomatic enteritis [20]. In FMF, the suppression of caspase activity by pyrin is disrupted, thereby leading to an increased production of inflammatory cytokines, including IL-1β [8, 21]. Some reports have suggested that IL-1β induces IL-23, which is involved in refractory IBD [22, 23]. In addition, in IBD, inflammasomes, which secrete NLRP3, IL-1β, and IL-18, is involved in intestinal inflammation and fibrosis [24]. Colchicine has been demonstrated to inhibit the NLRP3 inflammasome and suppress caspase-1 activation in gout [25]. Therefore, colchicine also exhibits therapeutic potential in managing sigmoid colon ulcers and strictures.
Based on this case of a patient with sigmoid colon stricture who was successfully treated with colchicine after FMF was diagnosed following CD, the possibility of FMF should be considered when periodic exacerbations are observed.



Comments (0)