Multiple cancer disease refers to that in which more than one malignancy is diagnosed in the same patient, either simultaneously or sequentially. In patients with multiple cancers combined with esophageal cancer, a highly curative treatment such as that in the present case may be provided by choosing a staged operation, if necessary, in view of the operation time and degree of invasiveness. To achieve a better therapeutic effect, careful preoperative surgical planning is necessary, along with a multidisciplinary treatment plan that includes high-intensity preoperative chemotherapy and nutritional therapy [9, 14].
The overlap between malignant esophageal disease requiring SE and hepatobiliary pancreatic disease requiring PD is very rare. Any additional digestive surgeries, especially resectional procedures, performed after a prior SE or PD can be extremely difficult. The cases of simultaneous or metachronous SE and PD in the same patient are very interesting from both a scientific and a practical viewpoint. When divided chronologically, there are three possible clinical scenarios. The first is when the two diseases are noted simultaneously, the second is when PD is needed after SE, and the third is when SE is needed after PD. For the first clinical scenario, there are only 11 reported cases of esophageal and biliopancreatic tumors occurring simultaneously and requiring distal esophagectomy (DE) or SE and PD (Table 1). All of these cases required very long operative times and tended toward heavy bleeding, indicating that they are highly invasive procedures. When two malignant lesions are noted at the same time, as in this clinical scenario, it is possible to consider preoperatively whether to perform a simultaneous resection or a multi-staged resection, and there are multiple options for the treatment strategy. As shown in Table 1, 5 of the 11 cases were selected for two-staged surgery, and six underwent simultaneous resection. However, in almost all cases in which simultaneous resection was performed, DE was performed only via a transhiatal approach, and Ivor Lewis reconstruction was also performed [15,16,17]. In contrast, staged surgery tended to be chosen for cases requiring a more invasive thoracic approach, such as SE and McKeown esophagectomy [18,19,20,21]. Of the five patients who underwent staged surgery, SE was performed in the first surgery and PD in the second surgery in four of these patients. In some cases, the reason for choosing this sequence is that the order is determined by factors that affect the degree of tumor progression and prognosis [22]. There are also reports that SE was performed first due to concerns about postoperative complications, especially pancreatic fistula after PD [19]. Another advantage of splitting the thoracic and abdominal manipulations into two-staged surgery is that the first operation can focus on tumor resection and lymph-node dissection, whereas the second operation focuses on gastrointestinal reconstruction along with abdominal dissection [20].
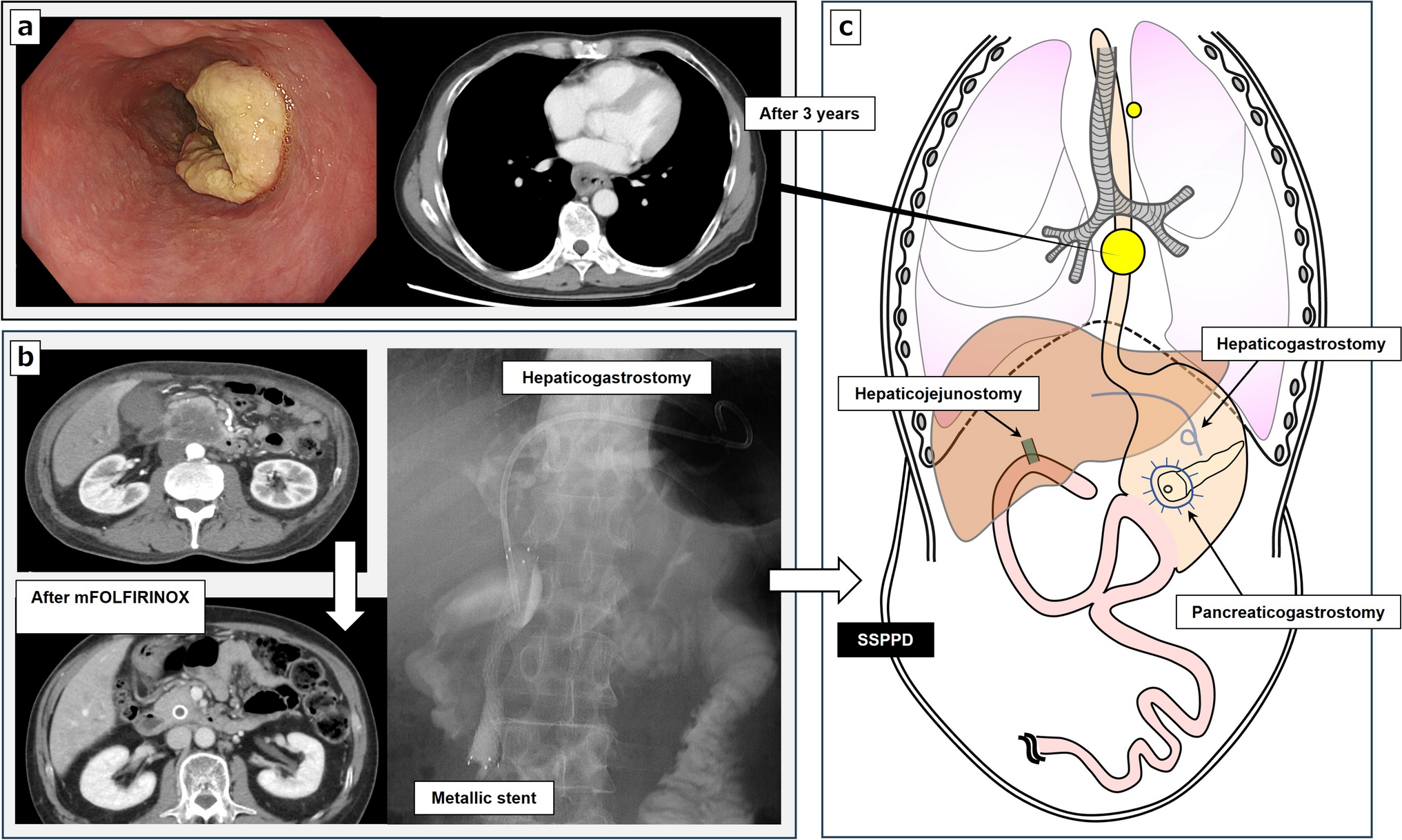
Table 1 Case series in which esophagectomy and pancreatoduodenectomy were necessary due to synchronous malignanciesIn the second and third clinical scenarios, the need for SE and PD occurs heterochronically. The treatment strategy is limited by the need for atypical procedures with respect to lymph-node dissection and reconstruction methods, because these two surgical interventions significantly alter the normal anatomical relationship of the upper abdomen. The second clinical scenario, in which PD is required after SE, is not rare, and a relatively large number of reported cases are scattered throughout the literature [23,24,25,26]. As shown in Table 1, in almost all cases of staged resection for simultaneous cancers, the sequence of SE first, followed by PD, was chosen in almost all cases, which confirms that this surgical sequence is not impossible. However, the third clinical scenario, for which disease requiring SE was noted after PD surgery, was reported extremely infrequently, with only five cases, including our case and one case of benign disease (Table 2) [27]. Only three cases of SE required cervical gastrointestinal anastomosis, which is more invasive than DE, including the present case, and all were limited to 2019 or later [28, 29]. Two important oncological points are worth mentioning in our case. One is that both pancreatic head and esophageal cancers were highly advanced, and high-intensity chemotherapy, such as mFOLFIRINOX, TS-1, and DCF, were used in the perioperative period for each disease, with the earlier PD being a conversion surgery, whereas radical lymph-node dissection was required for the later SE. The other is that the PD reconstruction procedure performed prior to SE was a pancreaticogastrostomy. This has never been reported before to our knowledge. If the esophageal cancer is an early stage cancer, as reported by Morikawe et al. [29], one-stage reconstruction with SE using robotic surgery may be possible, or a single resection and reconstruction may be possible for DE for esophagogastric junction cancer [30]. If the cancer is advanced, as in the present case, and long-term chemotherapy is required, we believe that choosing a two-staged surgery will improve oncologic safety. Because of the shortage of jejunum available for reconstruction due to Child’s reconstruction for PD, the right hemicolon is generally supposed to be suitable for esophageal reconstruction. A colon graft can easily be brought up to the neck without microvascular anastomosis, making it a favorable procedure [31]. However, jejunal interposition offers functional advantages, because it more closely resembles the esophagus, and the versatility of the jejunal flap is useful in solving various complex scenarios [16]. In addition, in our presented case, extensive colonic adhesions near the hepatic and splenic flexures complicated the colon reconstruction.
Table 2 Case series of esophagectomy after pancreatoduodenectomyTo the best of our knowledge, this is the first report to describe minimally invasive SE for advanced esophageal squamous cell carcinoma after SSPPD with pancreaticogastrostomy for advanced pancreatic head cancer. The decision on surgical technique in this patient was very difficult, and we planned a two-staged surgery after a thorough preoperative review. In conclusion, the procedure reported here may be recommended as an option for staged resection and reconstruction in patients with simultaneous advanced esophageal cancer after PD. The use of complex surgery in the treatment of cancer patients has made reoperations challenging. However, staged surgery options exist, and meticulous preoperative planning and intraoperative judgment can help the surgeon to perform an extensive and successful oncologically sound procedure.



Comments (0)