Our study analyzed the clinical features and long-term outcomes of 38 patients with cSLE with serositis (20.54%) from a cohort of 185 patients with cSLE. Pediatric patients with SLE with serositis had a younger age at SLE diagnosis, higher disease activity during serositis diagnosis, a higher rate of PICU admission, a higher prevalence of LN, CNS lupus, ESRD, and a higher SLICC/ACR damage index score than that of patients without serositis. The patients with cSLE with serositis also had low complement levels and high anti-dsDNA titers, indicating high disease activity during the presence of lupus serositis. Our results are consistent with those of previous studies showing higher disease activity in adult patients with SLE with serositis [6, 23]. In contrast to that in adult patients, we did not observe a significant association between serositis and cardiovascular events in patients with cSLE [10].
Although pleuritis and pericarditis are common cardiac and pulmonary manifestations of SLE, the primary diagnostic priority in our patients was to exclude infection, especially pneumonia or systemic infections. The combination of antinuclear antibodies (ANA) positivity (titer ≥ 1:80) and decreased C3 and C4 levels in pleural effusions demonstrated a sensitivity of 82%, specificity of 89%, and a negative predictive value of 93% for distinguishing lupus pleuritis from non-lupus exudative pleural effusion [24, 25]. In contrast, adenosine deaminase (ADA) activity was significantly elevated in infection-related pleural effusion [24]. A study of 2390 patients with SLE demonstrated that hemolytic anemia, proteinuria, lymphadenopathy, and anti-Sm antibodies were associated with pericarditis, while anti-DNA antibodies were associated with both pericarditis and pleuritis [23]. Pleuritis was also found to predict later gastrointestinal infarction or resection and was associated with long-term organ damage in SLE [23]. In our cohort, 31.57% of our patients with cSLE having serositis were diagnosed with serositis at the time of their SLE diagnosis, aligning with findings from previous studies comparing pericardial manifestation in adult- and childhood-onset SLE [26]. Additionally, half of our patients developed serositis within 1 year of their SLE diagnosis.
While adult patients with SLE with serositis receive increased methylprednisolone pulse therapy and higher maintenance doses of glucocorticoids [27], a higher percentage of our pediatric patients with lupus serositis received cyclophosphamide and methylprednisolone pulse therapy for high disease activity or deteriorating renal function due to LN. Notably, 72 (38.91%) patients with cSLE in our cohort received rituximab, and the percentage of rituximab use was similar in patients with and without serositis. The use of rituximab as an add-on maintenance therapy for LN has been shown to decrease the cumulative maintenance dose of glucocorticoids and achieve more favorable LN control according to our previous study on cSLE [28].
Despite aggressive treatment, significant comorbidities, and death (39.47%) occur in patients with serositis. In patients with cSLE with serositis who expired, the median time from serositis diagnosis to death was 99 days. One-third of these patients died 1 month after the onset of serositis, and 66.66% died within 6 months after serositis onset. Septic shock and ICH are leading causes of death in patients with serositis. In addition to Gram-negative bacteria-related sepsis, fungal and Pneumocystis jirovecii opportunistic infections also contribute to mortality, suggesting a fulminant course due to the immunocompromised status. The risk factors for severe infections, ICH, and high disease activity in our patients with serositis included bone marrow suppression after immunosuppressant use and prolonged leukopenia, lymphopenia, thrombocytopenia, and ESRD. In contrast to our previous study on cSLE, which showed that the most common form of CNS lupus was ischemic stroke [29], the current study showed that ICH was more common in patients with cSLE and serositis. Increased incidence of ICH may be related to the combined effects of systemic inflammation, thrombocytopenia, high lupus activity, and severe infection in patients with SLE [30].
A recent study showed that the 10-year survival rates were 90.2–93.2% for adult SLE and 98.9–100% for cSLE in a medical center in Taiwan [31]. However, there is a high percentage of loss to follow-up in this retrospective study. Our previous study showed a mortality rate of 27% of all cSLE patients from 1985 to 2005 in our hospital [29]. In this study, we further showed that the overall mortality of patients with cSLE had much improvement to 10.81% in the recent 20 years.
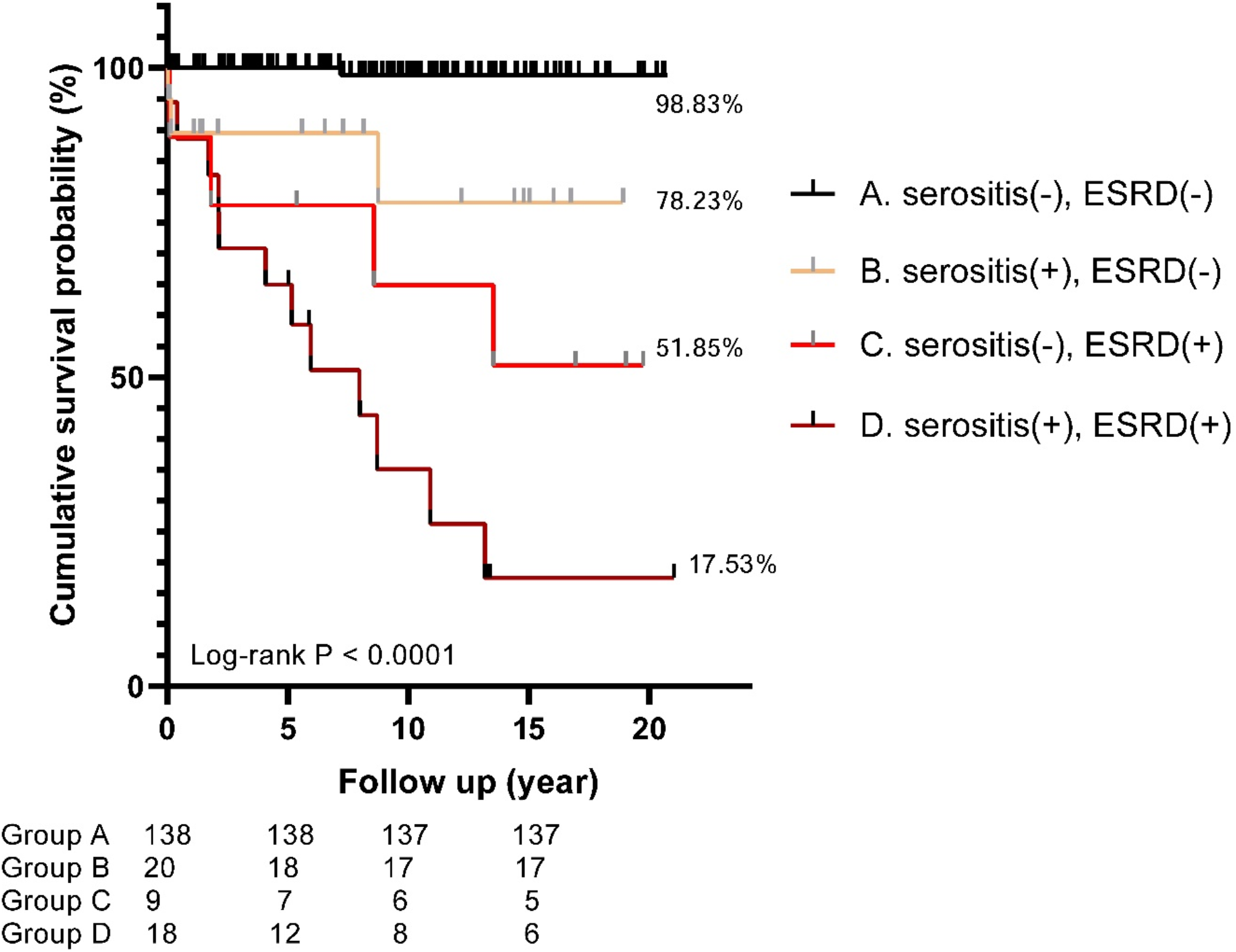
Our study demonstrated that lupus serositis, particularly in the late-onset group, and ESRD are significantly associated with mortality, consistent with Chen et al.‘s study on pericarditis in adult SLE [32]. Previous studies have shown fibrinous pericarditis with immunoglobulin, C1q, and C3 deposition in the walls of the blood vessels of the myocardium and pericardium, as observed through direct immunofluorescence [33,34,35]. Severe inflammation and immune complex-mediated injury in myocardial and pericardial tissues, as noted in autopsy findings, correlated with marked clinical and serological disease activity in SLE [34]. Pericarditis in SLE can present as a chronic process, an isolated attack, or recurrent brief episodes. The development of heart failure is often associated with pericarditis, hypertension, fluid retention due to renal disease, or corticosteroid use [36]. In addition to ESRD, which has a significant impact on the survival of patients with both adult- and childhood-onset SLE [37, 38], other poor prognostic factors for mortality include higher daily doses of corticosteroid, chronic kidney disease, and severe infections [31]. Previous studies on adult SLE showing a favorable prognosis for SLE-related serositis primarily focused on serositis occurring at or shortly after the diagnosis of SLE, similar to the patients with early-onset serositis in our study [9, 39].
Our study had several strengths, including the accuracy of SLE diagnosis and the inclusion of data on comorbidities, causes of death, and factors associated with survival. Our study also had some limitations, including a small sample size and a retrospective study design. We may have only reported serositis with effusion more than 0.5 cm in depth in a medical center, which potentially limits the generalizability of our results to the entire cohort. The findings of this study should enhance the clinicians’ awareness of the negative impact of serositis on cSLE outcomes.



Comments (0)