Study design, data sources
The Department of Adult Psychiatry and Psychotherapy as part of the Psychiatric University Hospital of Zurich, is responsible for the psychiatric inpatient treatment of adult patients in the City of Zurich, Switzerland, and its surroundings, with a catchment area of approximately 500,000 inhabitants. Our study retrospectively analyzed electronic health records of all travelers admitted and discharged from our hospital between January 1st, 2013, and December 31st, 2020. We extracted routine clinical data from electronic health records for the present study. The Ethics Committee of the Canton of Zurich authorized the use of the anonymized data for research and publication purposes (BASEC: 2018 − 01906).
We used sociodemographic, clinical, and service use variables for the present analysis. Sociodemographic variables included age, sex, marital and educational status, German language proficiency, migration status, and country of origin. The clinical variables we used were the main treatment diagnoses according to the WHO-ICD-10 criteria; the Clinical Global Impression Scale (CGI); and the Health of the Nation Scales (HoNOS). In addition, we extracted the pharmacological and non-pharmacological treatments prescribed during the hospitalization from the clinical records. Service use variables included the type of admission, admission ward, duration of treatment, type of discharge (i.e., regular or irregular in case of discharge against medical advice, court decision, death, or suicide of inpatients), and transfer to another hospital. Travelers were defined as such if they had their permanent residence outside Switzerland and were not registered as asylum seekers. For propensity score matching each admitted traveler was matched to one Swiss national patient and to one migrant patient. Domestic migrants without Swiss nationality were selected as a separate comparison group in order to better consider factors such as a foreign home country, foreign language or cultural peculiarities as confounders. Migrants were hereby defined as people without Swiss nationality who have permanent residence in Switzerland and are legally registered and insured as such. This includes, for example, registered asylum seekers during their asylum procedure or after being granted residence status or immigrants from other countries residing in Switzerland.
In order to obtain representative and sufficiently large groups of patients, we classified the treatment diagnosis upon discharge in six diagnostic groups according to the ICD-10 categories [20]: Alcohol and Substance Use Disorder (F1) Schizophrenia Spectrum Disorders (F2), Mania and Bipolar Disorder (F30-F31), Major Depressive Disorder (F3X), Anxiety and Stress-Related Disorders (F4-F5), and Personality Disorders (F6). Furthermore, we recorded the presence of comorbid alcohol and substance use and personality disorders.
The Clinical Global Impression (CGI) Scales and the Health of the Nation Outcome Scales (HoNOS) were rated upon admission and discharge. The CGI is an easily applicable measurement instrument to assess severity (CGI-S) and improvement or deterioration during hospitalization (CGI-I). CGI-S is rated on a seven-point Likert scale from 1 (“normal”) to 7 (“extremely ill”). The CGI-I evaluates changes in comparison to the previous CGI evaluation. It ranges from 1 (“very much improved”) to 7 (“very much worse”), whereby a score of 4 indicates no change [21, 22].
The HoNOS is a measurement instrument used to assess the severity of psychiatric disorders in 12 different domains covering behavior, symptomatology, impairment, and psychosocial functioning. Each item is rated on a five-point Likert scale from 0 (“no problem”) to 4 (“severe to very severe problem”). We evaluated the HoNOS at scale level (i.e., sum score ranging from 0 to 48) and item level [23,24,25,26]. We considered HoNOS Items rated three or four as clinically significant and as an integral part of the patients’ care plan [26].
Statistical analysis
According to the principle of independence, the analysis only included the first admission between January 1st, 2013, and December 31st, 2020. Descriptive statistics (mean, standard deviation, median, interquartile range - IQR, and percentages) were used to characterize the travelers admitted to the hospital during the observation period.
We used the propensity score to represent the probability of individual cases to be a traveler, conditional on their observed characteristics. Using logistic regression, we determined the relationship between travelers and sociodemographic and clinical characteristics, and service use patterns. Odds ratios (OR) were calculated with a 95% confidence interval (CI). Therefore, categorical variables were dichotomized, allowing to assess the risk associated with a single condition in contrast to the absence of this specific condition.
In a further step, we calculated the propensity score using logistic regression with the sociodemographic, diagnostic, clinical characteristics, service use patterns of patients upon admission. Conditional on the propensity score, the distribution of observed baseline covariates will be similar between travelers, Swiss nationals, and migrant (with a residency status) patients, allowing to assess the unbiased effect of traveler status [27].
Each admitted traveler was matched to one Swiss national patient, and to one migrant patient. Thus, leading to final 1:1:1 ratio. For the calculation of the propensity score we included demographic variables (age, sex, education, German language proficiency, marital status); provenience (German speaking country, neighbor-country, Schengen-country or other Continent of origin); clinical (diagnosis, comorbidity, clinical severity, clinical characteristics); and service use variables (type of admission; type of admission ward; time of the day at admission). This was conducted based on their nearest neighbor on the propensity score scale; with the smallest absolute, averaged propensity score distance across all included subjects [28, 29]. If no matching pair was found, cases were excluded to guarantee similar distribution of variables in the secondary dataset.
To assess the balance between the groups (before and after matching), we used the standardized mean difference (SMD) for continuous variables, the Chi-square (χ2) test for proportions, as well as propensity score distribution before and after matching. We conducted an equivalence test for statistically different variables with a low effect size to determine whether the observed effect was smaller than our smallest effect size of interest (SD = 0.50). We chose a half standard deviation since it is consistently considered as a minimally important difference in health outcomes [30, 31]. Two separated one-sided tests were performed to determine if the observed effect was greater than the lower bound (i.e., SD > − 0.50) and less than the upper bound (i.e., SD < + 0.50). Equivalence can be stated when the confidence interval lies within the equivalence boundaries [31,32,33].
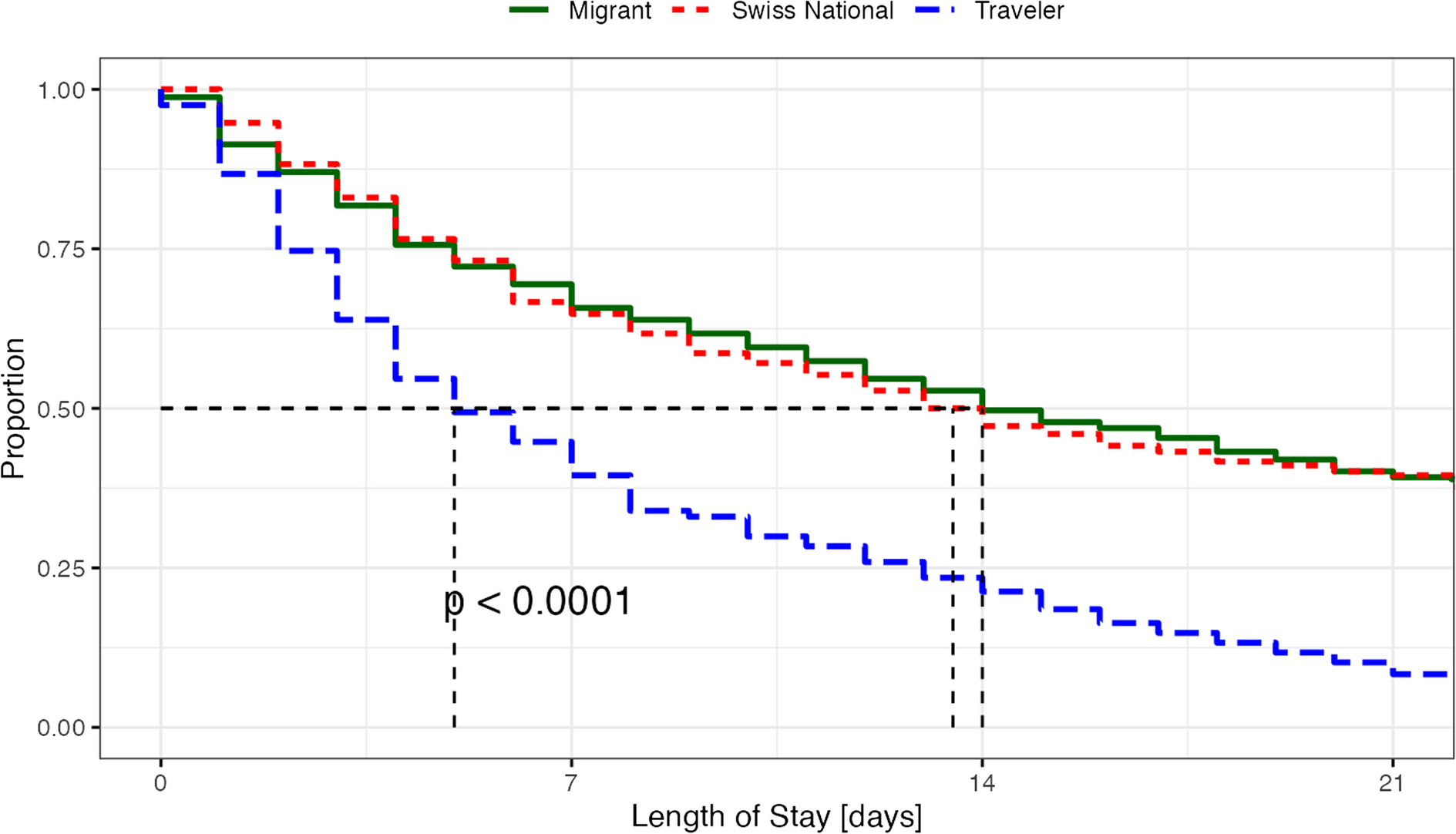
All subsequent analyses were conducted with the propensity score-matched sample. Variables measured at discharge were used to estimate the differences in treatment prescribed and outcomes between compulsorily and voluntarily admitted patients. We used analysis of variance (ANOVA), with a subsequent pair wise Student’s t-test to assess differences in continuous variables and the Chi-square test (χ2) for differences in proportions. For changes in HoNOS sum scores, from admission to discharge, a single-factor independent group analysis of covariance (ANCOVA) was used to test for differences according to the migration status (i.e., traveler, Swiss national and migrant), thereby controlling for variability in scores upon admission. Kaplan-Meier time-to-event curves representing time to discharge (i.e., duration of treatment) was calculated; for testing the statistical significance, we use the log-rank p-value.
All tests of significance were two-tailed. Due to the large sample size, p-values less than 0.05 were considered significant. For significant results, SMD was used to evaluate effect sizes. For the analysis of the single HoNOS items, a Bonferroni correction for repeated measurements was performed. Because all remaining analyses were considered exploratory, no further correction for multiple comparisons was performed.
Statistical analyses and figures were conducted using RStudio (2024.04.0 + 402); the statistical software R (4.1.2); and the R packages: tidyverse (1.3.1), TOSTER (0.3.4), MatchIt (4.3.1), survival (v 3.2–13), and survminer (0.4.9).




Comments (0)