This study aimed to identify factors influencing unintended nephrostomy catheter dislodgment (NCD) after placement, with cortex-to-skin distance shortening emerging as a key determinant.
Unintended NCD is a frequent complication with a wide incidence range. NCD occurred in 26%, 36%, 53%, and 62% of patients (n = 283) at 6, 12, 24, and 36 months after placement, respectively [19]. The clinical burden is significant, requiring time-intensive re-interventions that increase patient discomfort, radiation exposure, and healthcare costs [8, 14, 20]. NCD is implicated in 52–79% of catheter malfunction cases [4, 9, 21]. Its high frequency and risks underscore the need for effective prevention.
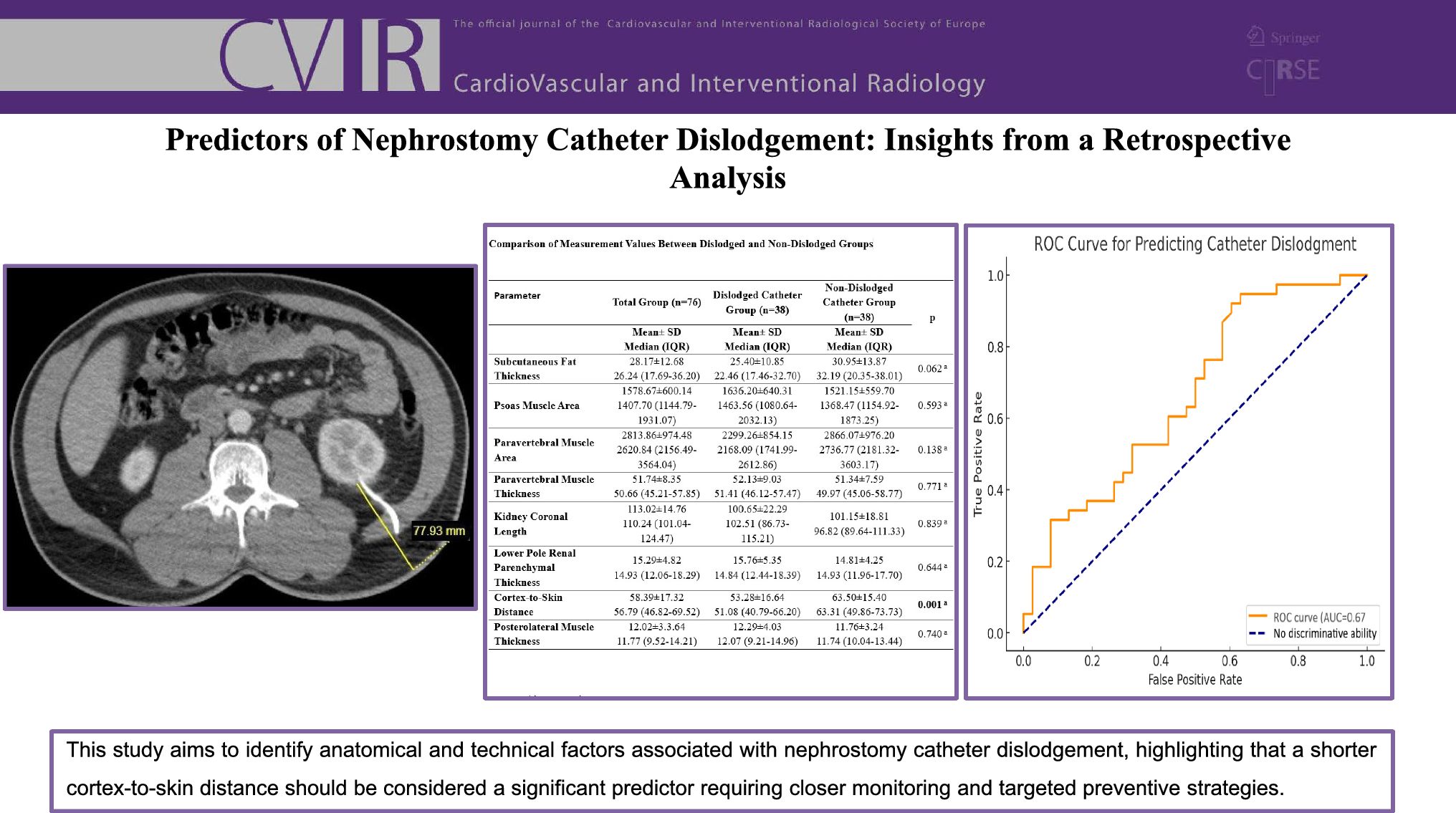
The nephrostomy catheter traverses multiple anatomical layers, including skin, subcutaneous fat, abdominal muscles, retrorenal and perinephric fat, and renal parenchyma, to access the collecting system [22]. This study identified the cortex-to-skin distance as a critical factor. A threshold of 46.65 mm was associated with a significantly elevated dislodgment risk. Shorter distances may reduce stabilizing forces, increasing susceptibility to NCD. Patients above this threshold had a reduced risk, supported by high sensitivity (92.1%).
However, specificity (39.5%), positive predictive value (60.3%), and AUC (0.67) highlight the limitations of this metric alone. High sensitivity aids in identifying at-risk patients, but low specificity results in false positives, potentially leading to unnecessary monitoring or interventions. Thus, cortex-to-skin distance should be interpreted within a broader clinical framework.
The moderate predictive performance (AUC = 0.67) underscores the importance of a multifactorial approach. Including clinical and procedural variables—such as age, sex, comorbidities, body composition metrics, and catheter fixation techniques—may enhance predictive accuracy. Anatomical differences influenced by age and sex, like variations in muscle mass and fat distribution, could affect catheter stability. Comprehensive models incorporating these factors are crucial for more robust risk stratification.
Future studies should focus on integrating anatomical, demographic, and procedural factors into risk models. This could improve understanding of NCD mechanisms and support strategies to enhance patient outcomes. Other parameters, including muscle thickness, subcutaneous fat thickness (p = 0.055, borderline significance), and renal parenchymal thickness, were not significantly associated with NCD in this study. However, the cortex-to-skin distance provides essential anatomical insights into catheter stabilization.
Patients with shorter cortex-to-skin distances may benefit from enhanced monitoring or adjunctive fixation techniques, such as hub sutures or securement devices, to mitigate NCD risk. Clinical application of these findings could help optimize catheter stability and improve outcomes.
The role of BMI in catheter dislodgment remains inconclusive, with conflicting evidence in the literature. Some studies associate higher BMI with increased NCD risk, while others report no significant correlation [13, 15]. Our study did not match for BMI in propensity-score adjustments, as doing so might have obscured key anatomical differences, such as muscle composition and other body structure metrics, which are central to our investigation of NCD risk.
Our results contrast with David et al., who reported a higher BMI in dislodgment cases (mean BMI: 39.7 vs. 30.9 in controls) [15]. However, their study used larger catheters (Malecot, Modified Foley) after percutaneous nephrolithotomy (PCNL) with tract dilatation, whereas our study utilized standardized 8F pigtail catheters without prior dilatation. Furthermore, their predominantly obese cohort may have been influenced by biomechanical factors such as flank pannus mobility, which were less relevant in our cohort (mean BMI = 25).
Conversely, our findings align with Navarrete et al., who found no significant association between BMI and NCD in a cohort primarily composed of oncology patients with pigtail and Foley catheters [13]. In contrast, Alam et al. reported BMI-related dislodgment but included patients with malignant ureteral obstruction, prior surgeries, radiation therapy, or infections—factors excluded in our study to minimize confounding [8].
These differences highlight the context-dependent nature of BMI's impact on NCD and emphasize the need for larger, BMI-stratified studies to clarify its role in catheter stability.
Preventive strategies for patients with shorter cortex-to-skin distances include regular catheter checks, use of self-locking catheters, securement devices, and timely replacements [9, 12, 13, 23,24,25,26]. Given the relatively low specificity and AUC of cortex-to-skin distance, incorporating additional factors such as patient demographics, comorbidities, and catheter care practices into risk models is essential for better identification of high-risk patients.
Limitations
This study has several limitations. The retrospective, single-center design and relatively small sample size may restrict the generalizability of our findings. The reliance on age and sex as matching variables, while justifiable due to their availability and clinical relevance, may overlook other potential confounders, such as comorbidities or catheter care practices. Although BMI would have been a useful variable for propensity-score matching, it was not included in our study due to data limitations, which may have affected the balance of unmeasured confounders. Additionally, the inclusion of imaging parameters, such as paravertebral and psoas muscle measurements, was exploratory in nature, and their lack of significance highlights the need for further validation in larger cohorts. Variability in procedural techniques among multiple operators and the absence of data on catheter care practices and patient education levels further limit the study’s scope. Addressing these limitations through prospective, multicenter studies with standardized protocols could provide a more robust understanding of the factors influencing catheter dislodgment.








Comments (0)