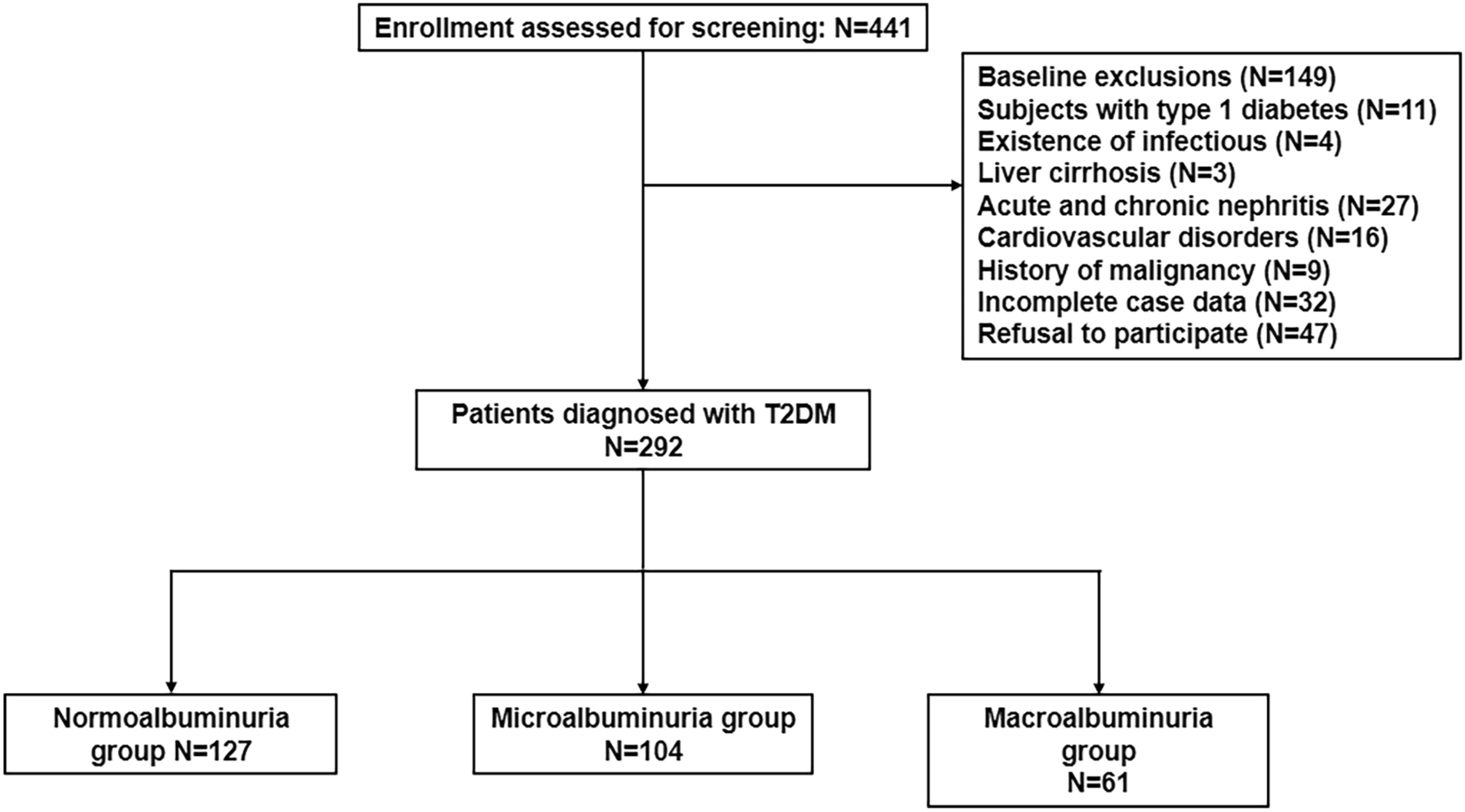
In this multicenter, single-arm, phase 4 study conducted at 15 sites in India, the safety and efficacy of Gla-300 was evaluated in 220 insulin-naïve people with T2D over 24 weeks. The study also fulfills the regulatory requirement of conducting a phase 4 clinical trial requiring evaluation of outcomes in more than 200 Indian participants.
The results support the outcomes reported from other international Gla-300 studies, including the BRIGHT and EDITION 3 RCTs [12, 17] and the DELIVER Naïve, DELIVER Naïve D, ATOS, and Toujeo-1—real-world evidence (RWE) studies [20, 23,24,25]. The mean age of participants in the current study was less than that reported in other RCTs (54 vs. 58.2 and 60.6 years) [12, 17] and RWE studies conducted in Asian populations [26].
Safety Outcomes
The safety profile of Gla-300 in the current study demonstrated that approximately 25% of participants reported AEs; nevertheless, the earlier studies have shown a similar safety profile with no new safety concerns observed [20]. No treatment-related AEs were reported in this study; one participant reported an SAE, which was not related to the study treatment. The most frequently observed TEAEs by SOC (in > 2% of participants) were infections, general disorders and administration site conditions, gastrointestinal disorders, musculoskeletal and connective tissue disorders, and nervous system disorders. None of the AEs were fatal or led to study discontinuation. No deaths were reported in the study.
A patient-level meta-analysis of EDITION 1, 2, and 3 RCTs provided cumulative information on AEs, wherein no differences in the safety profile were recognized, and the rates of AEs noted across all three EDITION studies were similar. Around 57% of participants reported TEAEs in the three EDITION studies [13], while in the present phase 4 study, the AEs reported were much lower. Two interventional global real-world studies (REACH and REGAIN) reported incidence of anytime (24 h) hypoglycemia were low (33.4% and 37.2%, respectively) in the Gla-300 arm; Gla-300 was noted to be beneficial in nocturnal, symptomatic documented hypoglycemia and severe/symptomatic documented hypoglycemia. However, the TEAEs profile in both REACH and REGAIN studies was 59.4% and 60.5% participants, respectively, which was comparatively higher than the current study finding [16].
The pragmatic randomized ACHIEVE control study [27] evaluating Gla-300 in insulin-naïve adults with T2D reported a higher percentage of TEAEs than the current study (38% vs. 24.5%, respectively). Whereas the Toujeo‐1 [25] prospective, observational study evaluating Gla-300 in people with T2D uncontrolled on OADs also reported a higher percentage of SAEs during the study than the current study (2.1% vs. 0.5%, respectively). The most frequently reported SAEs in Toujeo-1 and the current study were similar. The head-to-head randomized BRIGHT study conducted in insulin-naïve people with uncontrolled T2D reported no specific safety concerns with Gla-300; it was well tolerated in the study population [17]. This finding is similar to the current phase 4 study conducted in the Indian population.
It is well established that the fear of hypoglycemia and hypoglycemia itself is a barrier to the management and treatment of diabetes. The possibility of hypoglycemia makes physicians and people with T2D less likely to initiate or intensify insulin dose, which again results in suboptimal glycemic control [28]. However, in the current study, Gla-300 was shown to be associated with instances of only level 1 hypoglycemic events (29.5%), and no level 2 or level 3 hypoglycemic events were reported. The symptoms associated with hypoglycemia reported in the current study were sweat, shaky trembling, drowsiness or dizziness, headache, heart-pounding, uneasiness, emptiness in the stomach, and fatigue.
Efficacy Outcomes
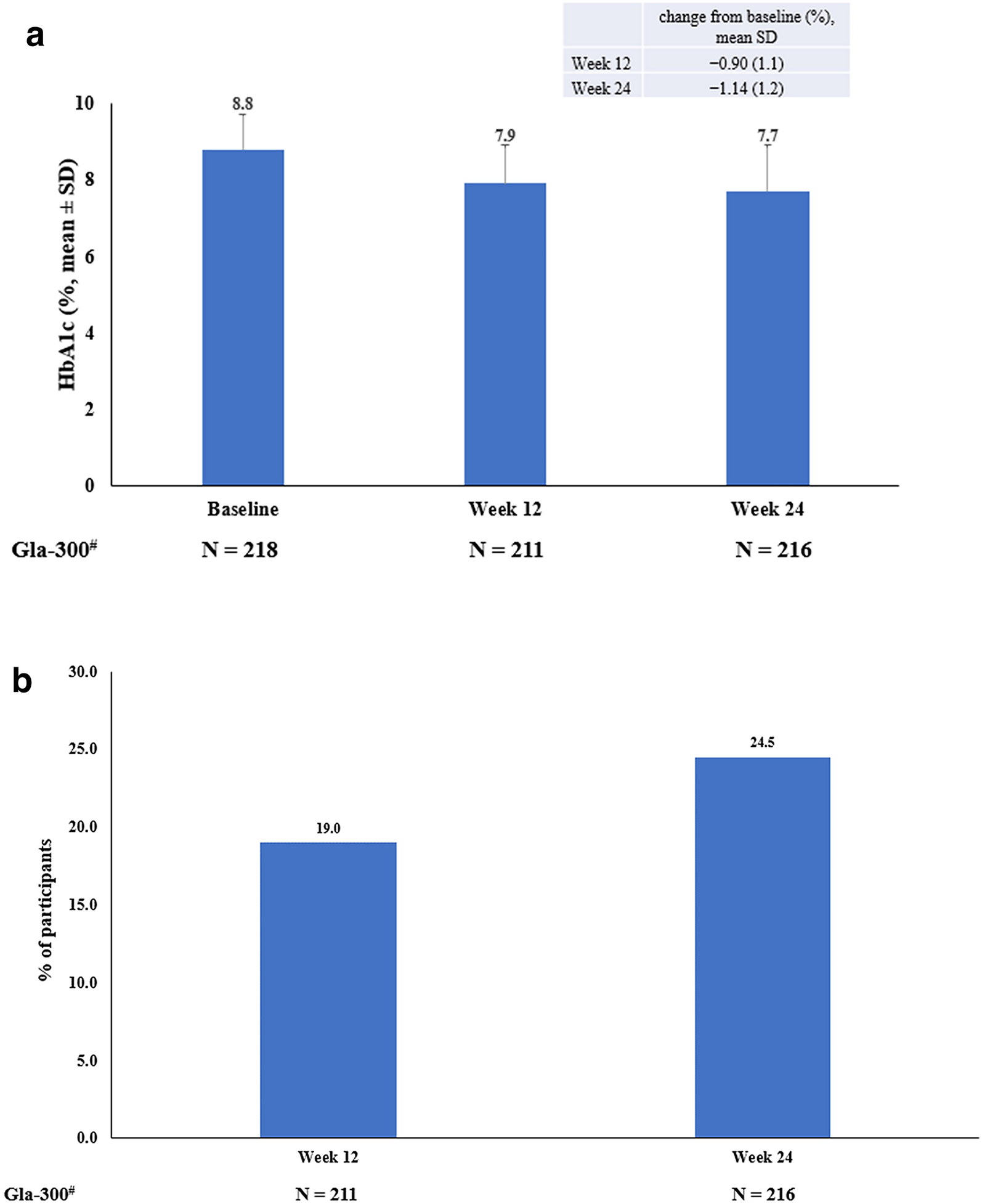
The present study demonstrated a similar improvement in HbA1c levels observed from baseline to weeks 12 and 24 (mean: − 0.90% and − 1.14%, respectively) to that reported in Toujeo‐1 (− 1.0% at month 6) [25]. However, the participants in the current study showed a slower improvement in glycemic control from baseline to week 24 of treatment in daily clinical practice than the participants in EDITION 3 [12] and BRIGHT [17] RCTs (at month 6: − 1.42% and − 1.64%, respectively), all three studies had similar baseline HbA1c levels (8.8% vs. 8.49% and 8.72%). This finding may be explained by the fact that in contrast to randomized controlled clinical studies, a less strict BI titration is employed in routine clinical practice. In DELIVER Naïve [23] and DELIVER Naïve D [24] real-world studies in insulin-naïve people with T2D from the US, greater reductions in HbA1c levels were observed at 6 months (− 1.52% and − 1.67%, respectively); however, in these studies, the baseline HbA1c levels were higher (9.6% and 9.7%, respectively).
In the present study, 19% and 24.5% of participants reached the HbA1c target of < 7% at weeks 12 and 24, respectively, which was similar to the values reported in the real-world ATOS study (25.2%), DELIVER Naïve (25.0%) [23], and DELIVER Naïve D (23.8%) [24]; however, it was lower than the values reported in EDITION 3 (43.1%) [12] and BRIGHT study (48.7%) [17]. This contrast may be attributed to the treat-to-target titration approach and more frequent follow-ups in the interventional studies, which resulted in better HbA1c target achievement. In the current study, the titration of insulin dose was done by the physician as per the locally acceptable titration algorithms. Nonetheless, it is implied that more frequent follow-ups with optimal insulin titration, improved therapy adherence, and the implementation of experimental programs are necessary to achieve controlled HbA1c levels.
An improvement in the 7-point SMPG profile was observed from baseline to weeks 12 and 24. However, the pre-breakfast reduction in the current study (− 39 ± 58 and − 48 ± 54 mg/dl at weeks 12 and 24 respectively); was in line with the findings of the EDITION 3 [12] study (at 6 months: − 3.35 ± 2.37 mmol/l).
In the present study, glycemic improvements in the form of reductions in both FPG and fasting SMBG values were observed at weeks 12 and 24. The average FPG levels at week 24 were on higher side in the current study than the ADA-recommended target FPG range (80–130 mg/dl), indicating that the majority of individuals require a more intensive treatment.
The observed improvement in glycemic control was achieved with a mean BI dose of 24.5 U/day and 29.9 U/day at weeks 12 and 24, respectively, which is lower than the Gla‐300 dose used in the BRIGHT study (50.5 U/day at month 6) [17]. These results imply that a larger number of participants could achieve optimal glycemic control with more intensive insulin dose titration, as seen in the previously conducted RCTs. Despite uncontrolled HbA1c, physicians’ and participants’ unwillingness to escalate therapy may have contributed to the insufficient up-titration of insulin dosages over the study period (clinical inertia).
The participants’ body weight stayed constant in the current phase 4 study, while it increased at month 6 in the real-world REACH trial [16], and EDITION 3 [12], and BRIGHT [17] RCTs (approximately 1.1, 0.5, and 2.0 kg, respectively). However, the findings of the current study are in line with the RWE studies, ATOS [20], and Toujeo‐1 [25]. The participants’ steady weight in the current study may have resulted from reduced insulin dosages, fewer hypoglycemic episodes, and lifestyle modifications.
In the present study, the treatment satisfaction measured using DTSQ scores increased from baseline to weeks 12 and 24, similar to DTSQ scores reported in the EDITION 3 study at month 6 (31.9). However, the change in DTSQs score from baseline was higher in the current study than that in the EDITION 3 study (10.2 vs. 4.9 at month 6). The difference can be attributed to the fact that EDITION 3 was an RCT, whereas the current study was a phase 4 study in an insulin-naïve population [12].
The current study assessed the safety and efficacy of Gla-300 in the Indian population, with a sizable number of participants with T2D for 24 weeks. This study adds to the body of evidence supporting the use of Gla-300, a second-generation BI analog, in the management of diabetes in this population. However, the current study was a single-arm, non-randomized, non-blinded study, wherein the participants were aware of receiving the new insulin therapy; this may have influenced their responses to the treatment satisfaction questionnaire and might have led to regression to the mean which cannot be excluded. Despite these inherent limitations, the current study from India found that Gla-300 use was associated with improved glycemic outcomes from baseline to weeks 12 and 24, as well as a low risk of hypoglycemia.



Comments (0)