
Remember me





Descriptive statistics for the study population with regard to the dimensions of the ASQ and SOC-29 are presented in Tables 1 and 2. A visual representation of the clients’ attachment profiles is shown in Fig. 3.
Table 1 Attachment styles and ASQ dimension scores among the study populationTable 2 SOC-29 scores among the study populationFig. 3
Attachment profiles of the study and reference populations
The clients exhibited moderate mean scores for four of the five dimensions of the ASQ (Table 1, Fig. 3). These dimensions included “confidence in self and others,” “discomfort in relationships,” “need for approval,” and “preoccupation with relationships.” The “relationships as secondary” dimension exhibited the lowest mean score.
The clients in the present study indicated a higher prevalence of insecure-avoidant attachments than the reference population. In the present study, the mean scores for “discomfort with relationships” and “relationships as secondary” were 0.8 and 0.67 points higher than the reference values, respectively. The present study population exhibited a lower prevalence of secure attachments than the reference population, with a mean score 0.65 points lower than the reference value. The prevalence of insecure-anxious attachments was slightly higher in the present study population than in the reference population, with differences of 0.10 and 0.03 points for the “need for approval” and “preoccupation with relationships” dimensions, respectively.
The clients’ mean SOC-29 score was 121. When adjusted for the number of items included in each dimension, the corrected mean scores were comparable across all dimensions. The highest score for the present study population corresponded with meaningfulness (MA = 4.69), and the lowest corresponded with comprehensibility (MA = 3.71) (Table 2).
Associations between attachment styles and SOC dimensionsThe correlations between attachment styles and SOC dimensions are presented in Table 3.
Table 3 Strength and significance of associations between attachment styles and SOCA secure attachment style was positively associated with total SOC and all three SOC dimensions, with significant and moderately strong associations between a secure attachment and total SOC, meaningfulness, and manageability. The association between a secure attachment style and comprehensibility was weak. Conversely, insecure attachment styles were negatively associated with total SOC and each of its dimensions. Generally, total SOC and manageability had the strongest associations with attachment style, demonstrating a moderate effect size with each of the attachment styles. The dimension of comprehensibility exhibited the weakest associations; its association with “relationships as secondary” did not reach statistical significance.
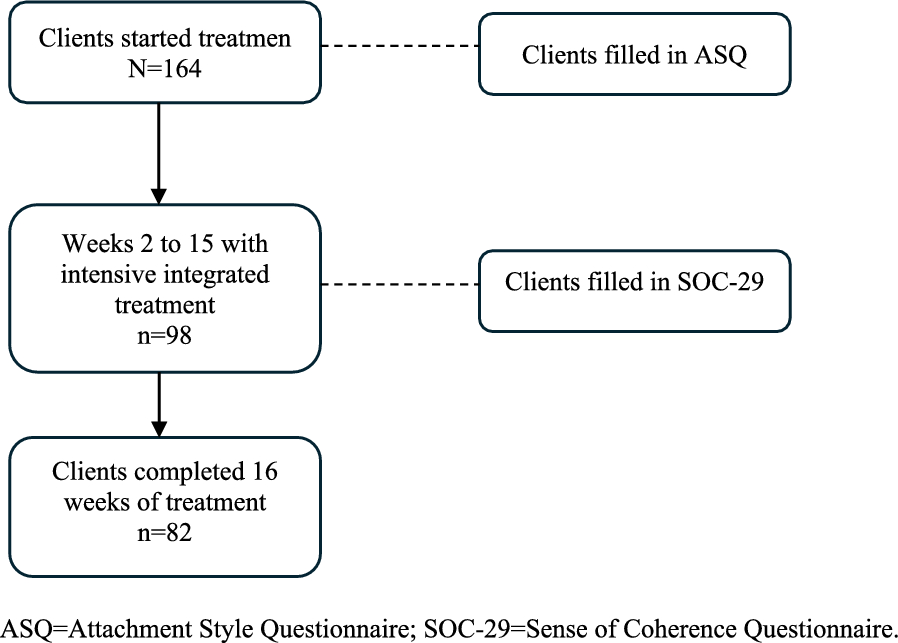
The predictive capacity of attachment styles and SOC for early dropout and treatment completionDue to the high dropout rate observed during treatment (40%), a logistic regression analysis was conducted to investigate whether any of the dimensions of the ASQ could predict early dropout. While none of the dimensions showed a statistically significant association with early dropout, “preoccupation with relationships” demonstrated a trend that neared significance (p = 0.07). Every 1-point increase in the “preoccupation with relationships” dimension was coupled with a 47% increase in the likelihood of a client dropping out during the course of the intervention (Exp[B] = 1.470).
In terms of predictive capacity for fully completing the intervention, no attachment style was found to have a significant predictive value. Similarly, the SOC dimensions of meaningfulness and comprehensibility did not demonstrate any significant predictive value. However, for each 1-point increase in manageability, there was a significant (p = 0.048) increase of approximately 10% in the likelihood of a client completing the intervention (Exp[B] = 1.097).
DiscussionThe clients in the present study predominantly exhibited an insecure-avoidant attachment style. This was particularly clear from the dimensions that assessed the need for interpersonal distance. While a minor elevation was also observed in one of the two dimensions associated with an insecure-anxious attachment, this deviation was minimal in comparison to the scores of the reference population [24]. This suggests that it is specifically an insecure-avoidant attachment style, not a general insecure attachment style, that is representative of the study population. However, the slight increase in insecure-anxious scores may support an overall insecure pattern, particularly when combined with the significantly elevated scores for the dimensions associated with an insecure-avoidant attachment. The insecure attachment style of the clients in the present study was further reinforced by their lower scores in the secure attachment style dimension in comparison with the reference population [24].
A higher prevalence of insecure attachments among individuals with SUD has been previously described [28]. Individuals with an insecure-avoidant attachment style often prefer to maintain distance from others and adopt coping approaches that depend less on other people [24]. They tend to avoid close relationships, which may serve as a protective mechanism against perceived vulnerability in relationships. As a result of adopting a generally distant and avoidant approach toward others, it may be reasonable to assume that individuals with SUD struggle to invest trust in care settings that rely on interpersonal relationships, including therapeutic relationships in the treatment of SUD, other forms of psychiatric care, and general healthcare. Considering that an insecure attachment may be a vulnerability factor for SUD and that SUD poses an elevated risk for comorbidities, attachment style potentially affects both the risk of developing SUD and one’s ability to engage in treatment [7, 29, 30]. Although the present study did not assess health-related treatment outcomes, its confirmation of a predominantly insecure attachment style among clients with SUD underscores the potential benefit of incorporating considerations of attachment style in the treatment of SUD.
Associations between attachment styles and SOC dimensionsGeneralized Resistance Resources (GRRs) and Specific Resistance Resources (SRRs) are fundamental constructs in the salutogenic theory, which emphasizes the promotion of well-being rather than solely focusing on disease treatment [11]. GRRs are broad, wide-ranging factors such as material resources, ego identity, and social support, which contribute to the development of a strong SOC. While GRRs are typically considered more generic, they can also manifest on an individual level, reflecting a person’s broader capabilities and resources that are not tied to a specific context.
In contrast, SRRs are more individualized and context-dependent, tailored to the person’s immediate needs and specific situations. In the context of clinical SUD treatment programs, SRRs might include a client’s particular coping mechanisms, therapeutic alliances, or access to program-specific resources. These resources enable the individual to effectively manage stressors within the unique environment of the treatment setting.
The salutogenic perspective considers the whole individual—physical, mental, emotional, and existential aspects—aligning with holistic approaches to care. By recognizing the interplay between GRRs and SRRs, care providers can better support individuals by leveraging both generalized and context-specific resources to enhance SOC, thereby promoting resilience and well-being during treatment.
The present study indicates that a secure attachment is positively associated, and insecure attachment styles are negatively associated, with overall SOC and all three SOC dimensions. A secure attachment style, characterized by confidence in oneself and others, can be considered a GRR. This is in line with the salutogenic theory and the definition of SOC—“…the extent to which one has a pervasive, enduring though dynamic feeling of confidence…” [11], p. 19). Individuals with secure attachments view themselves and others positively, facilitating better stress management and coping strategies. Overall, a secure attachment enhances both GRRs and SRRs and may act as an SRR in particular situations providing emotional support and fostering strong interpersonal relationships.
Previous research has highlighted the role of attachment styles in shaping SOC [31], which, in turn, may mediate the impact of an insecure attachment on subjective well-being [32]. Particularly notable in the context of adult clients with SUD are the significant and moderately strong associations between attachment styles and manageability, as shown in the present study. This suggests that manageability has the most pronounced influence on perceived health of the three dimensions of SOC. Previous studies have demonstrated that a more secure attachment style and a stronger SOC might have potential benefits for health and well-being [14, 29]; the current findings highlight the potential advantages of integrating interventions aimed at enhancing secure attachments and SOC into the treatment of SUD. The maintenance of good health requires the ability to effectively manage stressful situations [11]. Therefore, supporting individuals with SUD in strengthening their sense of manageability, helping them identify and utilize both personal and formal resources, is crucial. This support enables these individuals to effectively manage their situations and improve their health.
Moreover, SOC has been identified as a significant and central aspect of recovery capital, which encompasses both internal and external resources that support long-term recovery from SUD, including cultural, physical, human, and social capital. A moderately-to-strongly positive correlation between recovery capital and SOC suggests that strengthening SOC can equip individuals with additional resources to help them manage situations related to substance use [33]. By adapting a salutogenic perspective, individuals with SUD can develop a stronger SOC through coping strategies for better perceived health. Previous research has shown an association between improved SOC and better subjective health, including mental health, physical health, quality of life, and well-being [15, 34],this reinforces the positive effects of integrating a salutogenic perspective for clients undergoing interventions. From a care science perspective, an understanding of the possible impacts of attachment style and SOC on an individual’s preconditions for treatment and health has the potential to provide psychiatric and health care professionals with valuable insights into the individual’s coping mechanisms, thereby improving the conditions for tailored and person-centered care. This underscores the potential benefits of incorporating elements from these frameworks into interventions for SUD and future research to further explore their interconnectedness [17, 19].
Prediction of early dropout and treatment completionDuring the four-month, intensive, integrated treatment intervention for SUD, a substantial portion of clients opted to discontinue the program; 40% ceased treatment before completing the SOC-29 questionnaire. The observed correlation between early dropout and a predominantly insecure-anxious attachment style, notably within the “preoccupation with relationships” dimension, suggests that individuals who tend to excessively seek connection with others may not find this type of intervention suitable. However, it is important to interpret this result with some caution, as the correlation approached but did not reach significance (p = 0.07). While we cannot definitively explain why an insecure-anxious attachment was linked with early dropout from the intervention, a potential explanation may lie in the characteristic traits of this attachment style. Specifically, the dimension “preoccupation with relationships,” as described by Tengström and Håkansson [24], is characterized by an exaggerated fixation on relationships, where individuals seek intense contact to fulfill their needs for security in interpersonal connections. Given the intensity of the integrated treatment program, which involved active interventions five days per week [35], certain aspects of this format may have been overwhelming for these clients. Additionally, this group may have been particularly sensitive to staff turnover or other group-specific dynamics.
The link between attachment insecurity and challenges in SUD treatment is well-supported in the literature. Fletcher and Nutton [36] emphasized that individuals with insecure attachment styles often struggle with emotional regulation and interpersonal trust, which can adversely affect their engagement in treatment. Similarly, Cihan et al. [37] discussed the etiological role of attachment insecurity in the development and maintenance of substance use disorders. According to their work, insecure attachment patterns, including anxious-preoccupied attachment, may increase susceptibility to maladaptive coping mechanisms like substance use, particularly in the context of unmet relational needs.
Recent studies further support these observations. For example, Rübig et al. [38] demonstrated that insecure attachment patterns are highly prevalent among SUD patients and are associated with weaker therapeutic alliances and reduced therapy motivation, both of which are critical for treatment retention. These findings suggest that the insecure-anxious attachment style observed in our study may have hindered clients’ ability to engage effectively with the treatment program, contributing to early dropout. Similarly, Vismara et al. [39] found that preoccupied attachment styles, which are characterized by heightened dependency and emotional dysregulation, were more common among SUD outpatients compared to individuals in therapeutic communities, further highlighting the interplay between attachment patterns and treatment preferences or suitability. Interestingly, Fuchshuber et al. [40] noted that while attachment security is generally associated with positive treatment outcomes, it may paradoxically relate to early dropout in some contexts. This finding underscores the complexity of attachment dynamics in treatment settings and the need to consider individual differences in treatment planning.
Notably, treatment completion was significantly associated with the SOC dimension of manageability. This suggests that the intervention may have been demanding and stressful in terms of individuals’ abilities to manage their situations, since a higher manageability score was associated with an increased likelihood of a client completing the entire four-month intervention. Specifically, each additional point in the manageability dimension was associated with a 10% increase in the likelihood of treatment completion.
Comments (0)