Study setting
The present study took place at St. Paul’s Hospital, which is located in downtown Vancouver. St. Paul’s Hospital is a 400-bed acute care teaching hospital and is the provincial referral centre for a number of specialty surgical services, including cardiac surgery and gastrointestinal surgery. The hospital also offers various consulting services that are dedicated to managing pain and addiction. These include an interdisciplinary addiction medicine consult service, acute and complex pain services, and palliative care service.
In November 2019, Cerner, an electronic health record system (EHR) with computerized provider order entry (CPOE) system, was gradually rolled-out at St. Paul’s Hospital as well as other sites across the Lower Mainland region of British Columbia in an effort to provide more real-time data and consistent care to patients [29]. As part of the Cerner implementation, and relevant to this study, automatic stop dates were removed for opioid and benzodiazepine orders. Prior to Cerner implementation, orders would automatically be discontinued after 7 days for opioids and 30 days for benzodiazepines if a continuation order was not written by the prescriber. The Cerner system also allowed for the ordering of benzodiazepines days before short procedures (e.g., insertion of a peripherally inserted central catheter line, endoscopy, and bronchoscopy) with unclear discontinuation plans, a capability that was previously not possible.
Shortly after, in January 2020, Vancouver’s first opioid stewardship program was implemented at St. Paul’s Hospital. The opioid stewardship program is operated by a full-time clinical pharmacy specialist and a part-time addiction medicine physician, who were hired specifically with protected time to monitor active opioid prescriptions and provide audit-and-feedback recommendations, consultations, and educational activities related to the program and in-hospital opioid prescribing [31]. The audit-and-feedback component utilizes an automated screening algorithm as an initial screening approach to assist the clinical team in identifying potential high-risk opioid prescribing indicators. Shown in Table 1, thirteen patient- and prescribing-related indicators were adapted based on national and international clinical guidelines, research articles, and those developed by healthcare providers with pain-related expertise [6, 20, 30, 31], as well as availability of data elements in the pharmacy system used to generate the screening report. A shortlist of patients admitted to inpatient units, excluding the hospital’s critical care units or emergency department, and prescribed at least one opioid is generated. Following initial screening, those seen by the addiction medicine, palliative care, or the acute and complex pain services are excluded due to their distinct opioid needs and higher risks compared to the general population. Subsequently, remaining patients with the highest number of outcome indicators are selected to receive a full assessment by the clinical team. This approach allowed the opioid stewardship team to prioritize those in most need given capacity and time constraints with not being able to intervene on all patients who are at risk, and aims to optimize analgesic therapy and enhance pain management while prioritizing patient safety. The opioid stewardship team followed standard clinical pharmacy assessment by reviewing the patient’s chart and engaging in discussions with both the patient and primary care team. Any recommendations are communicated to the patient’s most responsible care team (through Cerner or verbally), documented in a Subjective, Objective, Assessment, Plan (SOAP) note format, with a follow-up assessment by the opioid stewardship program’s clinical pharmacy specialist within 72 h to determine whether the recommendation was accepted by the responsible care team.
Table 1 High-risk indicators for St. Paul’s hospital’s opioid stewardship programStudy sample
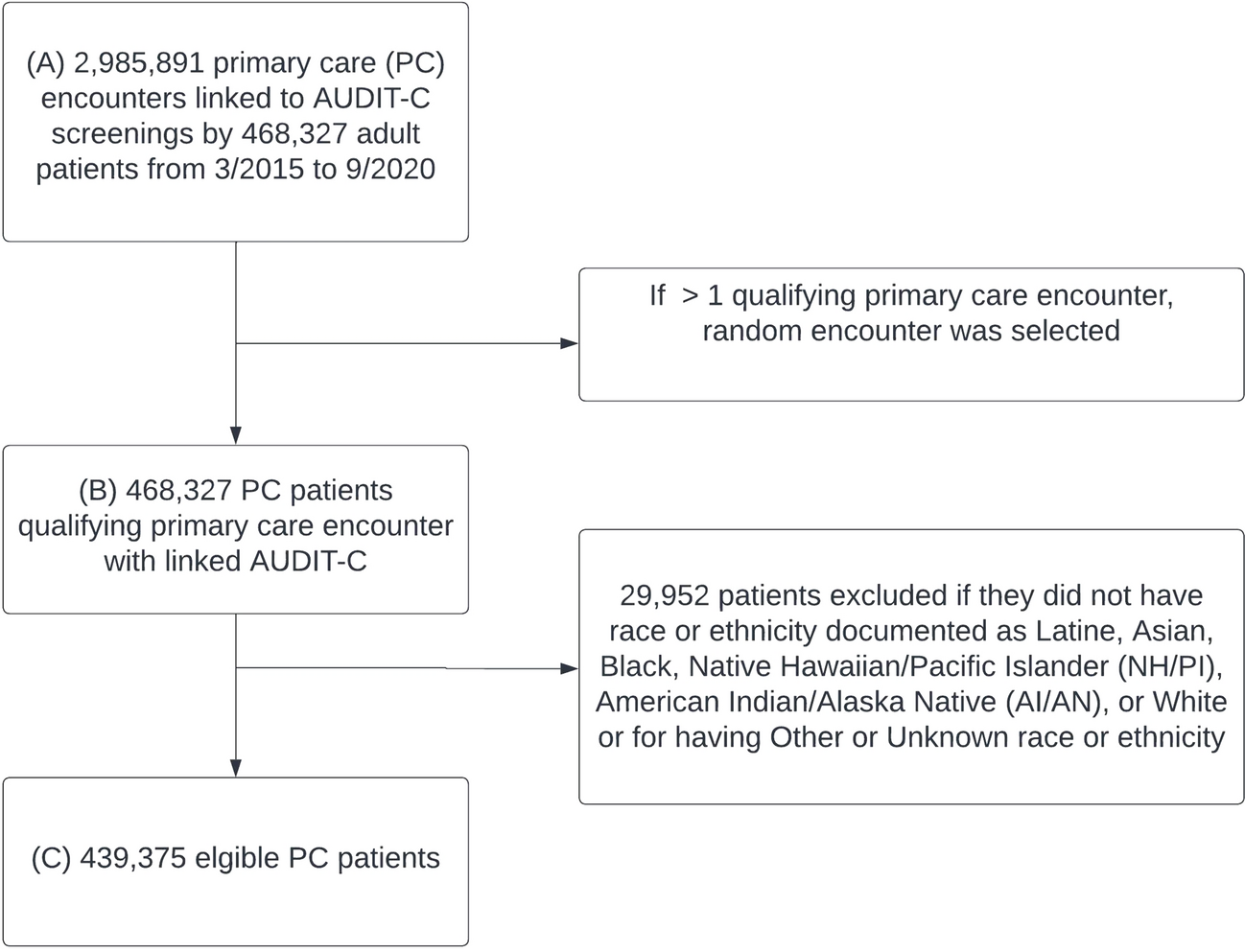
For the present study, we restricted to all patient encounters with an active opioid order admitted to St. Paul’s hospital, excluding those followed by emergency department, critical care, palliative care, acute and complex pain services, and addiction medicine. In order to account for pre- and post-opioid stewardship intervention, the study period was from January 2018 to March 2022, with the primary intervention date being January 2020.
Data sources and measures
We used three hospital data sources: (1) BDM Pharmacy database, which represented all hospital prescribing data prior to the implementation of Cerner (January 2018-November 2019), (2) Sunrise Clinical Manager, which contained scanned copies of all clinical chart notes prior to implementation of Cerner (January 2018-November 2019), and (3) Cerner (November 2019-March 2022) which contains both medication information and clinical records. To ensure data consistency and comparability across the two platforms prior to analysis, two pharmacy team members retrospectively manually coded all variables from the BDM Pharmacy database and Sunrise Clinical Manager to match those available in Cerner.
The primary outcome was the proportion of any high-risk opioid prescribing, based on having at least one of the 10 modifiable prescribing-related factors that were screened for at the time of assessment (Table 1). We also chose three individual prescribing-related factors to assess separately as secondary outcomes in an effort to tease out the potential confounding impact of Cerner on prescribing patterns. These included: 1) > 90MME high daily opioid prescribing; 2) continued opioid use on or after 5 days post-admission; and 3) concurrent opioid-sedative prescribing. We examined > 90MME high daily opioid prescribing given our hypothesis that this indicator would not likely be impacted by Cerner. Opioid use on or after 5 days post-admission and concurrent opioid-sedative prescribing were included as secondary outcomes given our hypothesis that the removal of automatic stop dates in the Cerner system would likely have impacted these two indicators, despite any potential beneficial effects from the opioid stewardship intervention. Ethics was obtained from the Providence Health Care/University of British Columbia Research Ethics Board.
Statistical analyses
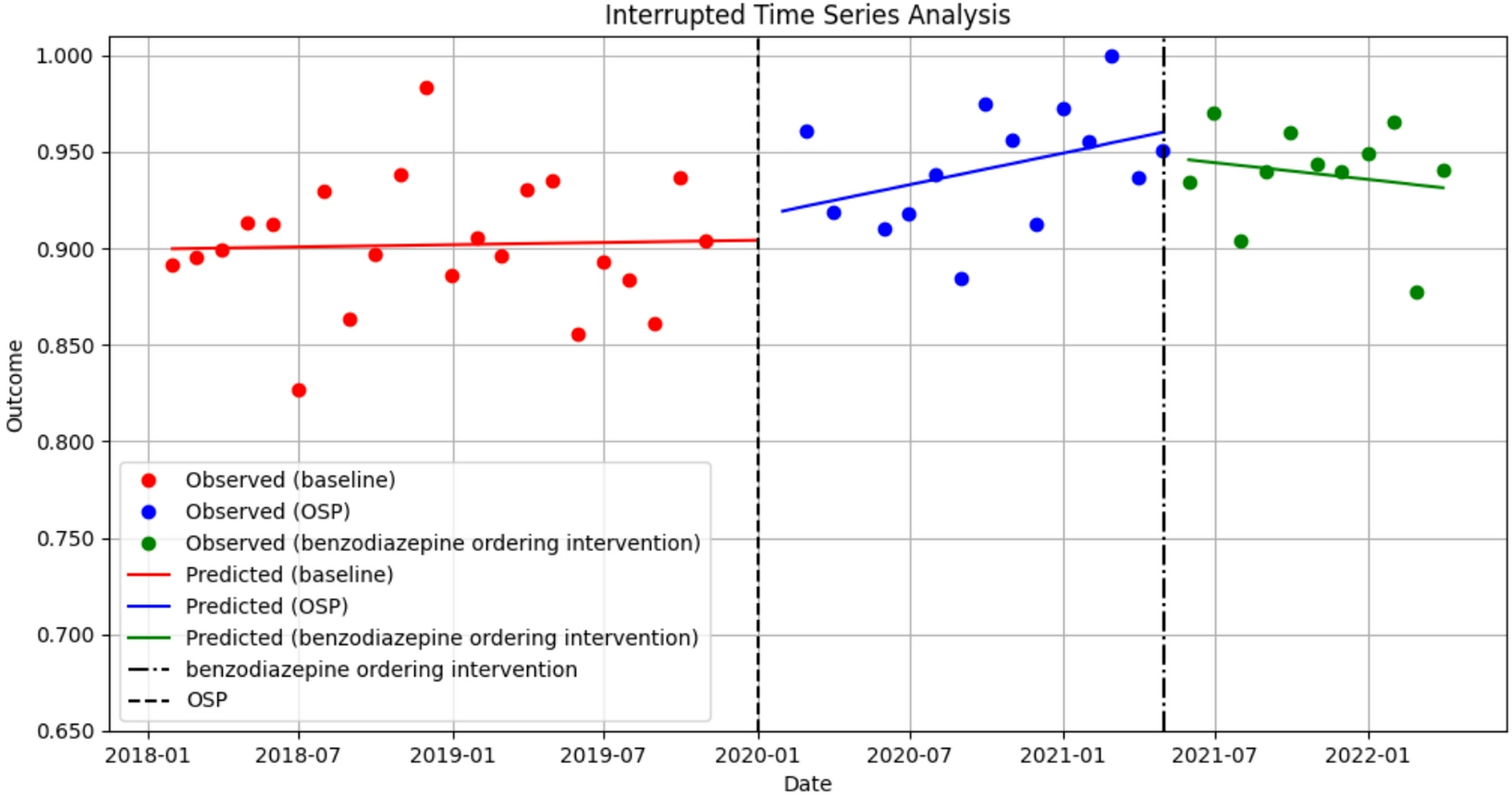
Using interrupted time series (ITS) analysis, we assessed the changes in the level and trend of our primary and secondary outcomes after the implementation of the opioid stewardship program. We utilized segmented regression with autoregressive integrated moving average error models, analyzed over monthly time points. In the present study, we collected serial cross-sectional data on the 15th of every month on every patient encounter who had an active opioid prescription over 49 time points (22 pre-intervention, 25 post-intervention). We used January 2020 as the intervention time point. Data for November and December 2019, and April 2020 were not available due to the electronic system switch to Cerner and an unanticipated pause in the program due to COVID-19, respectively. We assumed that the uptake of Cerner aligned with the opioid stewardship program intervention time point as it was rolled-out only a couple months prior. Given the unit of analysis was patient encounters, we adjusted for the fact that a patient could have multiple encounters in the ITS analysis. We assessed the presence of autocorrelation using the Durbin-Watson test.
We conducted a sensitivity analysis to assess the robustness of our findings, whereby the primary outcome, any high-risk opioid prescribing, was re-defined to remove the two indicators deemed sensitive to the Cerner roll-out (i.e., opioid use on or after day 5 post-admission, concurrent opioid-sedative prescribing). Following this, an ITS analysis was performed.
In additional analyses, we applied a multiple intervention ITS analysis to the concurrent opioid-sedative prescribing outcome, where we accounted for the subsequent interventions that occurred in May 2021 to reverse the unintended consequences of Cerner. As described earlier, Cerner allowed prescribers to order benzodiazepines days before a procedure as part of procedural powerplans (i.e., an electronic order set) with unclear discontinuation plans. In May 2021, efforts to adjust powerplans to ensure benzodiazepines were discontinued post-procedure specifically for gastrointestinal endoscopy, peripherally inserted central catheter (PICC) insertions, and bronchoscopy were implemented. These included review of workflow with the clinical teams responsible for these powerplans, and request to set a 24-hour duration on these procedural powerplans. All p-values were two sided with a significance level of 0.05. All analyses were carried out using Python V.3.12.






Comments (0)