Weight reduction following degenerative cervical spine surgery
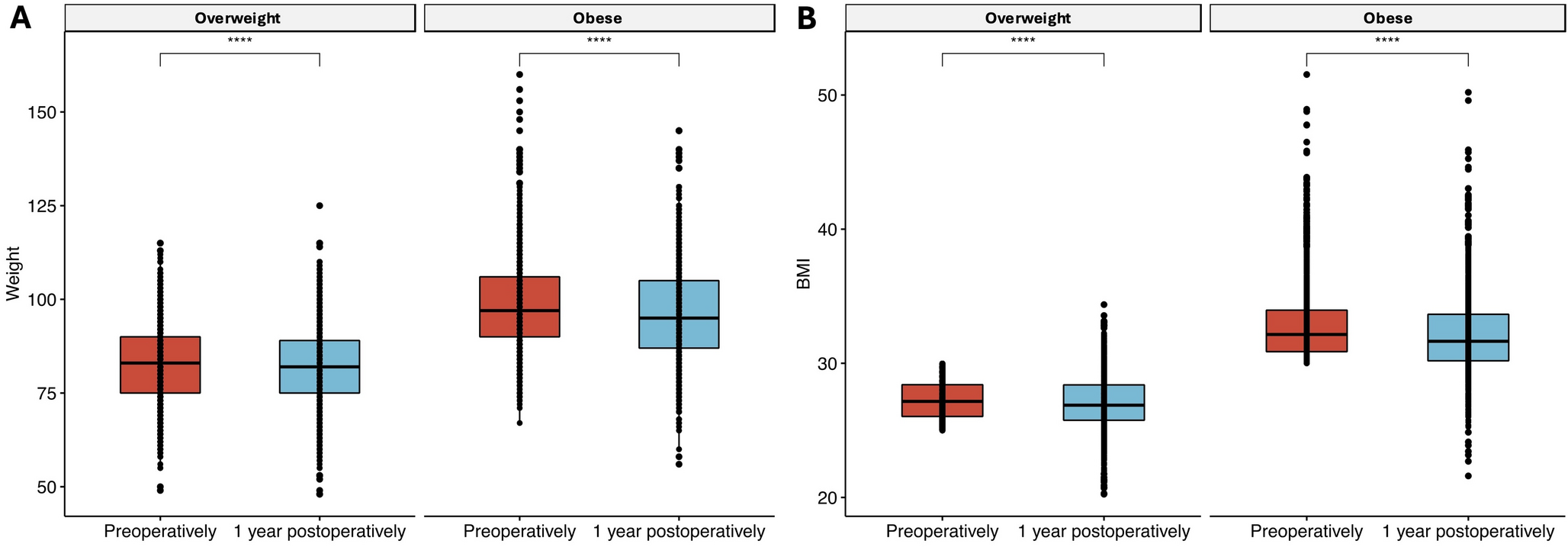
In this retrospective longitudinal cohort study, we observed a significant reduction in weight following degenerative cervical spinal surgery in obese and overweight patients. In fact, 19% and 22% of the total cohort had experienced significant weight loss (≥ 5% of initial weight) at 1- and 2-years postoperatively, respectively. The magnitude of weight loss in patients who experienced significant weight was approximately 7 kg and varied depending on the age and initial BMI, with younger and obese patients experiencing greater weight reductions. Also, following the surgery, around 20% of obese patients transitioned to a normal or overweight BMI bracket, while 12% of overweight patients reached a normal BMI.
This study suggests that while weight loss does occur, it is not universal among all patients undergoing cervical degenerative surgery. In fact, a smaller subset of patients experienced significant weight gain. Overall, weight loss appears to be more common and pronounced in specific patient subgroups, particularly those with higher preoperative BMIs and younger age.
A meta-analysis including 63 interventional trials investigating the placebo effect in weight loss trials, determined that on average, approximately 20% of patients with overweight or obesity in placebo groups experienced a ≥ 5% weight loss [15]. It is important to note that these placebo arms involved non-surgical, non-pharmacological, but strict interventions in the form of dietary counseling and physical activity. By comparison, in our cohort—comprising patients who underwent cervical degenerative spine surgery without participation in any structured lifestyle counseling program—20% of overweight or obese individuals similarly lost at least 5% of their initial body weight. This suggests that the impact of cervical degenerative spine surgery on body weight may be comparable to that of dietary lifestyle modifications implemented in a controlled and supervised trial setting.
As demonstrated in previous studies cervical degenerative spine surgery has been shown to improve patient-reported outcomes in terms of pain, function, and mobility [16]. These findings hence lend evidence to support our initial hypothesis that degenerative cervical spine surgery promotes weight loss by reducing pain, enhancing mobility, and increasing physical activity levels. Although somewhat conflicting and primarily focused on the lumbar spine, our findings are largely consistent with the limited research available on this topic. For example, a study by Akins et al. reported improved weight management one-year following lumbar spine surgery in obese and severely obese patients compared to non-obese patients, showing greater average weight loss in the severely obese group (3.2 kg) compared to the obese group (0.9 kg), which parallels our findings [17]. In addition, Vorster et al. (2023) conducted a meta-analysis of eight studies examining BMI changes before and after lumbar spine surgery. They found that obese patients were more likely to experience clinically significant weight loss compared to non-obese patients [8]. This contrasts with an earlier systematic review by Anderson et al. (2010), which included only two older studies and failed to provide consistent evidence of weight loss following lumbar surgery [18].
Similarly, Ross et al. published a retrospective analysis using a U.S. Veteran database in 2021, concluding that the likelihood of weight loss after spinal surgery for degenerative disease was no greater than that of weight gain. Ross et al. acknowledged the limitations of their findings, including variability in surgical procedures included in their study, which hindered the assessment of specific spinal locations and conditions. Furthermore, their study population primarily consisted of older male veterans, which may have limited the generalizability of their results [7].
To the best of our knowledge, no previous studies have explored the impact of degenerative cervical spine surgery on weight and BMI, making this study the first of its kind.
Factors positively associated with weight loss Post-Operatively
In addition to the previously noted association between higher BMI and significant weight loss, our findings revealed that younger patients were more likely to experience substantial weight loss, particularly within the first year following surgery. This observation aligns with recognized age-related factors, such as improved metabolism [19], enhanced physical recovery capacity, and better surgical outcomes [20, 21, 22], all of which can influence postoperative weight changes.
Moreover, we identified several key predictors of significant weight loss, including female sex, higher scores on the NDI, and elevated NRS pain scores. Our finding that females were more likely to lose weight is consistent previous studies showing that female sex was a psychosocial factor consistently linked to a greater potential for weight loss [23, 24, 25]. Potential explanations for this contrast may include variations in dietary habits, levels of physical activity, as well as differences in motivation and adherence to exercise regimens after surgery [26].
Moreover, the association of higher NDI and NRS pain scores with significant weight loss aligns with our hypothesis, indicating that these patients likely experienced pain relief and functional recovery following surgery, which may have contributed to improved mobility. Naturally, improvement in physical function from the preoperative baseline is more pronounced in patients with greater baseline impairments—those with higher neck disability indices. This is because individuals with more severe initial limitations have a greater capacity for noticeable recovery and potential improvement in physical function. In other words, this may have enabled these patients to re-engage in physical activities they had previously avoided, leading to greater motivation and better function for postoperative weight loss. Other factors such as heart disease, smoking, and surgical approach did not show a significant impact in our analysis.
Clinical implications
While some patients experienced significant weight reductions, the majority remained overweight or obese. Our study underscores the importance of integrated care approaches that combine surgical intervention with structured weight management strategies. Effective postoperative support, including physical rehabilitation and nutrition counseling, is essential for optimizing weight loss outcomes. Additionally, implementing strategies to motivate patients to adhere to medical advice and strengthen their support systems can significantly enhance weight loss and improve the long-term sustainability of results. Importantly, our findings can be used to counsel patients on the plausible weight-loss effects of degenerative cervical spine surgery and help set realistic preoperative expectations. Furthermore, identifying key predictors of significant weight loss can enhance preoperative counseling and postoperative management. Naturally, tailoring interventions to address the specific needs of these groups may increase the likelihood of achieving substantial weight loss.
Strengths and limitations including regression to the mean bias
A key strength of our study lies in the extensive Swespine registry, which encompasses 47 clinics nationwide. This established registry facilitates comprehensive data collection across multiple centers, enhancing the generalizability of our findings. The large cohort size further contributes to our statistical power, while robust data collection and analysis bolster the credibility of our results. However, this study has its limitations. The absence of data on physical activity and dietary changes restricts the ability to draw definitive conclusions regarding the factors and mechanisms influencing weight loss. While weight and BMI are crucial indicators, they do not fully capture changes in body composition, such as muscle and fat distribution, which could provide a more holistic understanding of health improvements. Additionally, full account of other confounding factors was limited, including socioeconomic status, medication use (e.g., corticosteroids), and other conditions that may affect weight change. Finally, while it is plausible that regression to the mean bias may affect the result of this study, the extent of weight loss was statistically significant and deviated from the expected evolution of weight in obese patients who do not receive any interventions, as described in other reports [27, 28]. Although the absence of a non-surgical control group limits the validity of these findings, previous studies suggest that spontaneous weight loss in obese individuals over several years is highly unlikely, with weights typically remaining stable over time in this patient group [27, 28]. Additionally, the proportion of patients undergoing a clinically relevant ≥ 5% weight loss is not insignificant (20%), which corresponds, as previously mentioned, to the proportion of patients experiencing weight loss as a result of encouraged dietary and lifestyle modifications [15].
Future research
Future studies should involve larger cohorts to evaluate the long-term sustainability of weight loss after spinal surgical interventions. As well as examine the effects of a comprehensive multi-professional approach that includes dietary factors and physical activity on weight, as well as specific patient characteristics that promote weight loss. It would be valuable to investigate factors that influence long-term weight sustainability beyond two years and to identify new predictive factors for weight loss on a larger scale and prospective manner. Finally, we hypothesize that surgical intervention enables patients—particularly those who were previously limited by pain or dysfunction—to resume physical activities, thereby contributing to weight loss. However, this remains speculative, and further prospective studies with more granular outcome measures are warranted to explore this potential causal pathway and to validate our findings.





Comments (0)