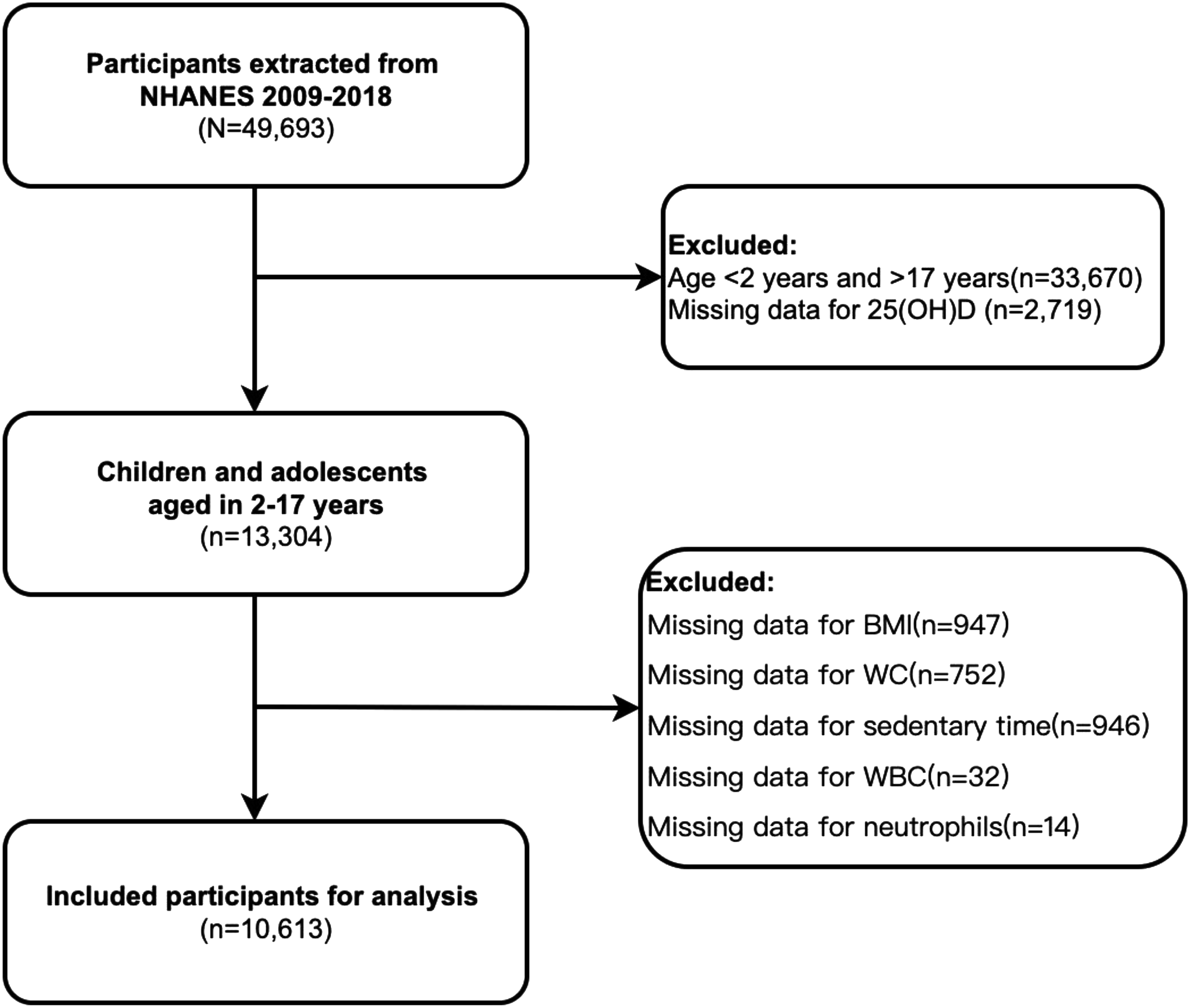
In this study, we evaluated the association between inflammatory markers, 25 (OH)D deficiency, and the risk of obesity in children and adolescents using data from five NHANES cycles (2009–2018). Our findings indicate that systemic immune-inflammation index (SII) and systemic inflammation response index (SIRI) are independently associated with an increased risk of obesity in this population, while 25 (OH)D appears to mitigate this risk. Additionally, all inflammatory markers neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), SII, and SIRI) exhibited a significant yet modest mediating effect on the relationship between childhood and adolescent obesity and 25 (OH)D deficiency. Specifically, NLR, PLR, SII, and SIRI contributed to the mediating effect in the inverse relationship between 25 (OH)D deficiency and obesity among children and adolescents, with mediation rates of 3.85%, 0.88%, 4.29%, and 1.29%, respectively. It is noteworthy that in this study, the ACME (average causal mediation effect), ADE (average direct effect), and total effects were all negative. This suggests that an increase in 25(OH)D levels is associated with a reduction in obesity risk, with inflammatory markers playing a mediating role in this relationship.
Association between 25(OH)D levels and obesity risk
This study demonstrated a significant negative correlation between 25(OH)D levels and the risk of obesity. Notably, after adjusting for age, gender, race, PIR, and waist-to-height ratio, individuals in the adequate 25(OH)D group exhibited a substantially reduced risk of obesity. These findings align with previous research; for instance, Vimaleswaran et al. utilized Mendelian randomization to establish that lower levels of 25(OH)D are linked to increased BMI and obesity risk, indicating a potential role for 25(OH)D in metabolic regulation [24]. Furthermore, Wang et al. reported a significant association between 25(OH)D deficiency and childhood obesity, suggesting that vitamin D supplementation may enhance metabolic health [25].
Potential mechanisms of 25(OH)D in obesityRegulation of adipose tissue
25(OH)D deficiency may influence the prevalence of obesity through several mechanisms. Firstly, vitamin D receptors (VDRs) are extensively distributed in adipose tissues, suggesting that 25(OH)D may regulate fat accumulation by modulating the differentiation and function of adipocytes [26]. This mechanism could explain the observed association between 25(OH)D levels and obesity risk.
Insulin resistance and inflammation
Secondly, a deficiency in 25(OH)D can lead to insulin resistance and chronic inflammation, both of which contribute to the development of obesity [27, 28]. Insulin resistance is a key factor in metabolic disorders, and chronic inflammation can exacerbate adiposity.
Anti-inflammatory properties
Additionally, 25(OH)D exhibits anti-inflammatory properties that can inhibit the release of pro-inflammatory cytokines, such as tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6), while promoting the production of anti-inflammatory cytokines like interleukin-10 (IL-10) [29]. Thus, 25(OH)D deficiency may exacerbate inflammatory responses, thereby increasing the risk of obesity [5].
Bidirectionality and future research
Numerous studies have established a negative correlation between low 25(OH)D status and obesity, as well as between obesity and 25(OH)D insufficiency or deficiency [30]. However, it remains unclear whether 25(OH)D deficiency leads to altered metabolism or whether the metabolic changes associated with obesity result in 25(OH)D deficiency [31, 32]. The findings of this study further underscore the potential role of 25(OH)D in the prevention of obesity.
Conversely, some research has indicated that low vitamin D levels could contribute to the development of obesity. The 11-year follow-up of the HUNT study revealed that individuals with lower baseline serum 25(OH)D levels exhibited a higher incidence of future obesity, demonstrating a 1.3-fold increased risk of abdominal obesity [33]. Additionally, epidemiological data from Norway indicated that serum 25(OH)D concentrations decreased in a gradient manner as body mass index (BMI) increased [34]. 25(OH)D is thought to influence various metabolic processes that regulate fat storage and energy metabolism. For instance, vitamin D receptors are found in adipose tissue, and their activation plays a role in adipocyte differentiation, lipid metabolism, and insulin sensitivity—key factors in the regulation of body weigh. 25(OH)D deficiency can impair mitochondrial oxidative capacity in skeletal muscle, reduce basal metabolic rate, and promote fat accumulation [35]. 25(OH)D plays a crucial role in maintaining insulin secretion by regulating calcium channels and vitamin D receptor (VDR) signaling. Low levels of 25(OH)D are associated with a decline in β-cell function [36].
Inflammatory markers and mediation analysis
This study indicates a significant association between 25(OH)D deficiency and elevated levels of inflammatory markers, such as the neutrophil-to-lymphocyte ratio (NLR) and systemic immune-inflammation index (SII). This suggests that 25(OH)D may influence the development of obesity by modulating the inflammatory response. Previous research has demonstrated that 25(OH)D possesses anti-inflammatory properties; it can inhibit the release of pro-inflammatory cytokines, including tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6), while promoting the production of anti-inflammatory cytokines such as interleukin-10 (IL-10) [37, 38]. Consequently, 25(OH)D deficiency may exacerbate the inflammatory response, thereby facilitating the onset of obesity. Their study suggests that the inflammatory response may play a mediating role in the relationship between 25(OH)D levels and metabolic health.
Some studies have indicated that no significant association exists between obesity and inflammatory markers [39]. However, it is widely accepted that childhood obesity is frequently associated with chronic low-grade inflammation, and these inflammatory markers are valuable in evaluating obesity and its related complications. For example, obese children often demonstrate elevated levels of NLR, PLR, SII, and SIRI, which indicate the presence of chronic low-grade inflammation in their bodies [40,41,42]. In obese individuals, structural changes occur in adipose tissue, accompanied by increased infiltration of immune cells, particularly macrophages, which sustain low-grade inflammation through the production of inflammatory mediators [43]. Furthermore, various cytokines secreted by adipocytes, such as IL-6, TNF-α, and C-reactive protein, stimulate immune cells, thereby triggering inflammatory responses [43]. These markers can be utilized to monitor inflammatory levels in obese children. The relationship between inflammation and obesity is widely recognized as complex and multifaceted [44]. Adipose tissue, which plays a crucial role in energy storage and metabolism, has the capacity to secrete various pro-inflammatory molecules. This secretion contributes to the establishment of a chronic low-grade inflammatory state commonly observed in individuals with obesity [45]. Such an inflammatory environment can disrupt normal appetite regulation and metabolic processes, ultimately leading to increased food consumption. This chain reaction can further exacerbate obesity, creating a vicious cycle in which inflammation and obesity mutually reinforce one another [45, 46]. The association between inflammatory markers and obesity underscores the necessity of considering inflammatory markers when assessing obesity and its related health implications.
The study found that both the Average Causal Mediation Effect (ACME) and the Average Direct Effect (ADE), as well as the overall effects, were negative. This suggests that higher levels of 25-hydroxyvitamin D (25(OH)D) are associated with a reduced risk of obesity. This finding implies that vitamin D may lower obesity risk through various mechanisms, including the modulation of inflammatory responses. Specifically, a negative ACME indicates that the inflammatory marker partially mediates the relationship between 25(OH)D and obesity, while a negative ADE suggests that 25(OH)D could influence obesity through additional, unmeasured pathways, such as the regulation of fat metabolism and enhancement of insulin sensitivity, among others.
This study demonstrates that inflammatory markers, specifically NLR, PLR, SII, and SIRI, have a partial mediating effect on the link between a deficiency in 25(OH)D and obesity. Significantly, the Average Causal Mediation Effect (ACME), Average Direct Effect (ADE), and total effects are all found to be negative, indicating that increased levels of 25(OH)D correlate with a reduced risk of obesity, with inflammatory markers acting as partial mediators in this relationship. Among these markers, NLR and SII displayed the most significant mediating effects, accounting for 3.85% and 4.29% of the associations, respectively (p < 0.001). These findings suggest that systemic inflammation might significantly influence the relationship between 25(OH)D deficiency and obesity. Inflammatory markers, such as NLR and SII, are widely recognized as reliable indicators of systemic inflammation and have strong associations with various metabolic disorders, including obesity and diabetes [47, 48]. For example, research conducted demonstrated a significant correlation between NLR and SII and childhood obesity, suggesting that elevated levels of these inflammatory markers may exacerbate obesity by promoting inflammation in adipose tissues and contributing to insulin resistance [28, 49, 50]. The findings of this study indicated that increased levels of SII and the Systemic Inflammation Response Index (SIRI) were associated with a substantial increase in obesity risk, further highlighting the crucial role of inflammation in the development of obesity.
Several studies indicate that elevated concentrations of vitamin D may significantly influence the regulation of inflammatory biomarkers in the body [51, 52]. In a controlled clinical trial, researchers observed a notable reduction in inflammation markers following a six-month period of vitamin D supplementation. This finding underscores the potential benefits of vitamin D in managing inflammation, suggesting that adequate levels of this vitamin could positively contribute to overall health by moderating inflammatory responses [53].
NLR and SII exhibit stronger mediating effects, while PLR and SIRI demonstrate weaker mediating effects. This discrepancy may be attributed to the distinct biological characteristics of these inflammatory markers and their mechanisms of action within the inflammatory response. Both NLR and SII are closely associated with the acute phase response. Neutrophils, when recruited to inflamed tissues, release inflammatory cytokines and reactive oxygen species, which result in tissue damage and further promote inflammation. This activation establishes a feedback loop in which inflammation perpetuates its own progression by attracting additional immune cells [54]. In contrast, the mechanisms associated with PLR and SIRI often seem less direct. Consequently, the insights provided by PLR and SIRI regarding inflammatory activity may be less pronounced, as these markers are likely more sensitive to general hematologic changes rather than to specific inflammatory responses [55]. NLR is a significant indicator of the systemic inflammatory response, representing the ratio between neutrophils and lymphocytes. Neutrophils are the first type of white blood cells to migrate to sites of inflammation, playing a pivotal role in the initial inflammatory response. In contrast, lymphocytes are essential for regulating immune responses. A higher NLR is generally correlated with a more pronounced inflammatory response, which may elevate the risk of obesity by exacerbating inflammation in adipose tissue and contributing to insulin resistance. SII not only reflects the quantity of inflammatory cells but also considers the role of platelets in inflammation. An elevated SII is correlated with various inflammatory diseases and may heighten the risk of obesity by fostering chronic inflammation and metabolic disorders. PLR primarily reflects the role of platelets in inflammatory responses. Although platelets significantly contribute to inflammation and coagulation processes, their impact on obesity may be relatively minor. This is likely because platelets are primarily involved in the later stages of inflammation, exerting a limited direct influence on obesity. While SIRI demonstrates certain sensitivity in assessing systemic inflammatory responses, its significance in obesity may not be as pronounced as that of NLR and SII. This discrepancy is likely due to the inclusion of monocytes in the SIRI calculation, as the role of monocytes in obesity-related inflammation is relatively complex.
This investigation explores, for the first time, the mediating role of inflammatory markers in the relationship between 25(OH)D deficiency and obesity in children and adolescents, providing novel insights into the interplay between vitamin D and obesity. Cross-sectional studies measure exposure and outcomes at a specific point in time, making it impossible to establish the temporal relationships between variables. Consequently, we cannot ascertain whether changes in 25(OH)D levels precede alterations in inflammatory markers or if these changes occur prior to the onset of obesity. This limitation in design implies that our findings can only indicate associations rather than establish causal relationships. To overcome this limitation, future research should consider adopting a longitudinal study design. Several studies have confirmed that the characteristic low-grade chronic inflammation observed in obese individuals is associated with 25(OH)D deficiency [27, 56, 57]. Furthermore, longitudinal studies can mitigate the impact of recall bias, as data is collected in real-time. Our findings suggest that vitamin D supplementation may play a role in preventing insulin resistance and improving systemic inflammation [58].
Study limitations
Despite the valuable insights provided by this study, several limitations should be acknowledged. The cross-sectional design of our study precludes the establishment of temporal relationships between 25(OH)D deficiency, inflammatory markers, and obesity. Therefore, our conclusions should be interpreted with caution and require further validation through longitudinal studies. Additionally, while our analysis adjusted for several potential confounders, residual confounding may still exist. Future research should consider additional variables that may influence the relationship between 25(OH)D and obesity. Although our study provides valuable insights into the mediating role of inflammatory markers in the association between 25(OH)D deficiency and obesity in children and adolescents, it is crucial to acknowledge that using a body mass index (BMI) threshold of ≥ 30 kg/m² as a criterion for obesity in individuals aged 2–17 years is methodologically inappropriate. This criterion may result in misclassification, which could potentially affect the interpretation of our findings. Future studies should employ appropriate pediatric BMI percentiles to ensure accurate classification and yield more reliable results.
Study novelty and contributions
This study retains a degree of innovativeness as it is the first to investigate the mediating role of inflammatory markers in the relationship between 25(OH)D deficiency and obesity in children and adolescents. The association between 25(OH)D deficiency and obesity involves complex metabolic interactions, including multiple mechanisms such as the inhibition of adipogenesis, regulation of energy expenditure, and control of inflammation. By elucidating the potential pathways through which 25(OH)D influences obesity, our findings offer new insights into the interaction between 25(OH)D and obesity. This research highlights the importance of considering inflammatory markers when assessing the impact of 25(OH)D on obesity risk.
Clinical implications and future research
Supplementing vitamin D may hold significant clinical potential for preventing and improving childhood obesity and its associated metabolic abnormalities. Given that obese children often exhibit lower levels of 25(OH)D, and that 25(OH)D deficiency is linked to an increased risk of obesity and its related diseases, appropriate vitamin D supplementation may enhance the health status of obese children. However, current research findings remain inconsistent, necessitating further randomized controlled trials to confirm the long-term effects of vitamin D supplementation in this population.




Comments (0)