In our study, vitamin A level was found to be low in 23% of the hospitalized patients. Vitamin A deficiency and subclinical deficiencies are still common worldwide, especially in Asia, Africa, Latin America, and Brazil. Approximately 250 million children younger than five years of age are estimated to have low vitamin A levels. It has been reported that 40–60% of children living in Africa face vitamin A deficiency [15]. Almost half of South East Asian school-age children have vitamin A deficiency [5]. Yet in India, this rate reaches 62% and leads to the death of 330,000 children annually [16]. Custodio et al. [17] in Brazil reported that 26.2% of school-age children had low vitamin A levels. Similarly, a prevalence study conducted in China reported that severe vitamin A deficiency was 5.16% and borderline deficiency was 24.29% [18].
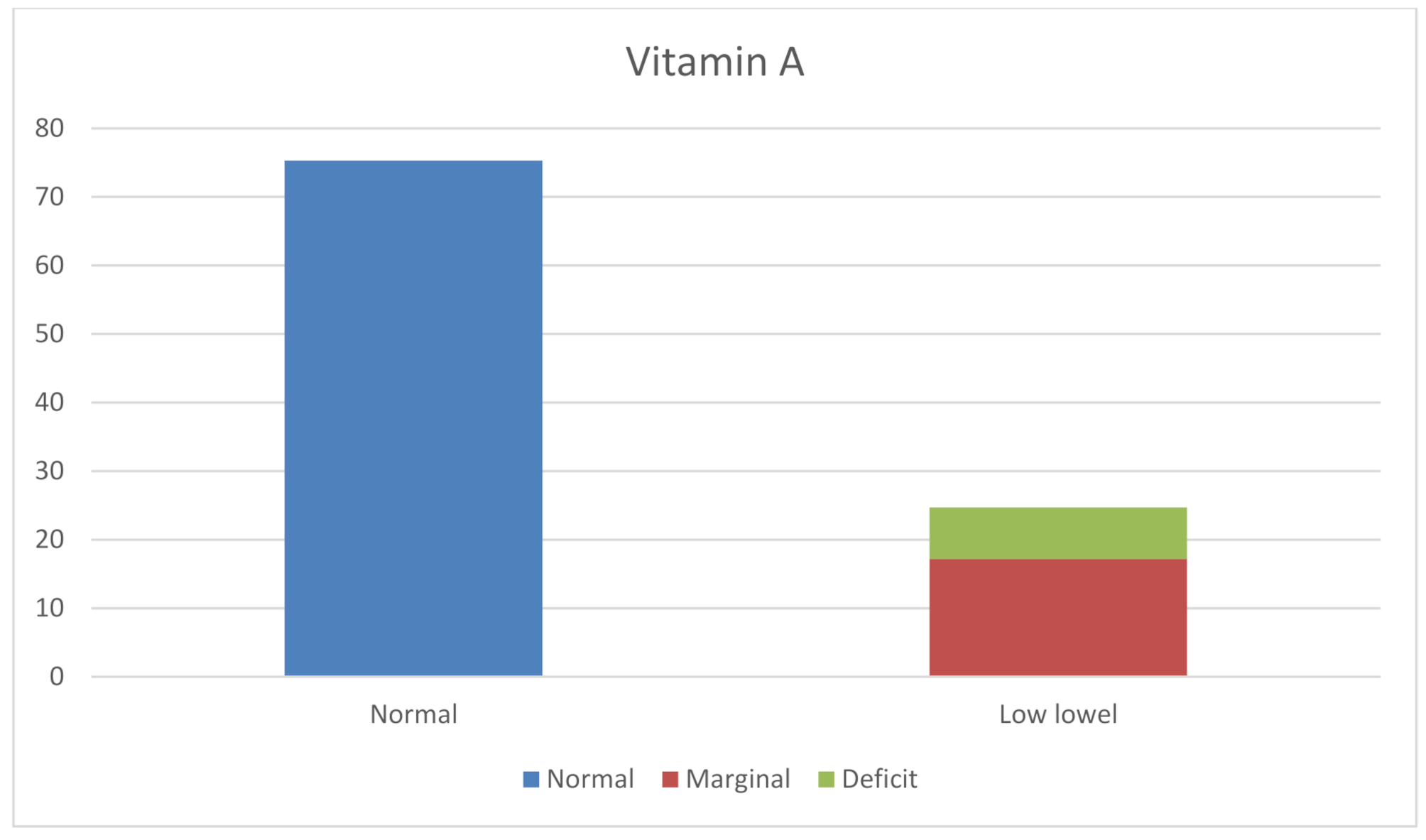
When we look at the vitamin A deficiency data in our country, according to UNICEF reports, the prevalence of subclinical deficiency under 6 years of age was reported to be 18% [9]. In the 2009 report of the World Health Organisation, it was reported that the prevalence of vitamin A deficiency in Turkey was 12.6%, and this was considered to be a mild public health problem [5]. Vuralli et al. [19] reported in a study conducted among 1063 healthy children aged 5–16 years in Ankara that there was no severe vitamin A deficiency, but subclinical deficiency was reported to be 2.2%. Again, Midyat et al. [20] reported that the mean serum vitamin A concentration was 283 ± 102 µg/L in children aged 29–54 months, and this ratio was positively correlated with weight-for-height measurements. In another study in which 100 healthy children between 36 and 48 months of age were evaluated, it was reported that vitamin A was found to be within normal limits in 89% [21]. Again in our country, in a study conducted by Wetherilt et al. [22], 11.6% of school-age children were reported to have vitamin A deficiency. According to the 2022 Turkish Nutrition and Health Survey data, this rate was reported to be 3–31% [11]. Our study shows that vitamin A is low in 33.6% of hospitalized cases and malnutrition accompanies some of them. The relationship between malnutrition and inflammation has been known for many years. In malnutrition, the catabolic vicious cycle such as decreased mucosal barrier functions and loss of appetite caused by the inflammatory response through cytokines in the organism leads to both decreased intake and loss of vitamin A [23,24,25]. Other micronutrient deficiencies, such as vitamin A deficiency, often occur as part of the malnutrition cycle [6]. The high level of vitamin A deficiency in our study may be explained by the fact that the hospitalized patients also had concomitant acute malnutrition. This situation indicates that malnutrition is still common in our country, and especially the nutritional status of hospitalized patients is poor. Although this study was conducted in a province in the westernmost part of Turkey which has a better socioeconomic status compared to other regions of Turkey, the fact that 23% of the patients had low vitamin A levels accompanied by a rather high rate of malnutrition indicates that there are still serious nutritional problems in our country. When our patients were evaluated in terms of cystic fibrosis, liver, and small intestine diseases that may cause fat malabsorption, with its feature of being a fat-soluble vitamin, one of the patients with low vitamin A levels was diagnosed with cystic fibrosis. Interestingly, 8 of our patients with levels < 316 µg/L were diagnosed with rheumatological diseases (3 with vasculitis and 5 with juvenile idiopathic arthritis). This suggests that chronic diseases may affect nutrition with long-term inflammation.
It has been reported that the rate of vitamin A deficiency decreases with increasing age. In our study, most of the patients with vitamin A deficiency were younger than 10 years of age. Similarly, Peige Song et al. [18] reported that vitamin A deficiency and marginal vitamin A levels gradually decreased with age. In another study from South Asia, it was reported that school-age children were more at risk for vitamin A deficiency [26].
Vitamin A (beta carotene-retinol) is an important fat-soluble vitamin involved in normal growth, night and color vision, and keratin production in skin, nails, and hair. Vitamin A can be taken directly from food (liver, fish oil, milk, butter, eggs) or from plants (dark green and yellow/red vegetables, carrots, apricots, broccoli, cabbage, etc.) in the form of beta-carotene which is converted into 2 molecules of retinal aldehyde and then absorbed. Vitamin A arriving in the liver is stored as a lipoglycoprotein in the form of retinyl esters. Normally, 300–900 mg is stored in the liver. Recommended Daily Allowance (RDA) suggests the daily required vitamin A retinol equivalent (RE) levels to be 400 mcg in 0–6 month infants, 500 mcg in 6–12 month infants, 300 mcg in 1-3-year-old children, 400 mcg in 4-8-year-old children and 600 mcg in 9-13-year-old children. According to the 2015 data of the Turkish Nutrition and Health Survey, it was reported that daily vitamin A intake in children in our country was lower than the recommended level of the RDA [10]. In the nutritional anamnesis of our patients with malnutrition, it was found that the consumption of eggs, green leafy vegetables, fish, chicken, red meat, and milk-dairy products was less than 4–5 times a week. As seen in our study, vitamin deficiencies are at a considerable level in patients hospitalized for various reasons [14]. In addition, low consumption of foods such as meat, fish, and chicken, which are the main protein sources, explains the malnutrition accompanying vitamin A deficiency found in the patients. In our country, many factors such as low socio-economic status and education level, inadequate food resources and their unbalanced distribution, wrong eating habits, and poor hygiene conditions lead to malnutrition and accompanying anemia, micronutrient, and vitamin deficiency. Considering the preventable serious complications, studies of hypovitaminosis of vitamin A and other vitamins provide the detection of clinical and subclinical cases and guidance in terms of evaluating the general condition [9,10,11,12]. The difference of our study from other studies is that vitamin A levels were evaluated in hospitalized patients, not in healthy children. Considering the high rates detected, it can be said that vitamin A deficiency is still a public health problem for our country.
The fact that our study was conducted only regionally does not reflect the data of our country. In addition, considering the additional problems that may accompany hospitalized patients such as malnutrition, these rates cannot be generalized accurately for the general population. These factors are the limitations of our study. However, our study can give an idea about vitamin A level and nutrition mistakes in hospitalized patients.
In conclusion, vitamin A deficiency may be observed in hospitalized children. These patients should be closely followed up in terms of nutrition education and vitamin supplements as a result of the diagnosis/treatment and prediagnosis of their primary diseases and detailed examination of their malnutrition status. A detailed evaluation of the nutritional status of each patient by pediatricians and acceptance of it as part of the examination will prevent both vitamin A and other vitamin deficiencies and malnutrition.




Comments (0)