Health-related quality of life and wellbeing are important narratives to judge the impact of a disease on affected people. In addition, the burden of disease is an additional aspect not only for people with the disease but also for the social environment and particularly for partners and/or families. Cultural beliefs and habits, as well as information about chronic diseases in a society may lead to differences in the perception of burden.
If a person is affected by a chronic stigmatizing illness, this brings a burden to partners and/or family. Psoriatic disease is a common condition for which there is no cure and patients, as well as their social environment, need to live and cope with it.
Surprisingly little is known about the life of partners of patients with psoriasis living in the same household. This may be because only few instruments have been described to measure hrQoL or burden in this important social environment [8]. Most data published have been generated by using the family dermatology life quality index (FDLQI), a generic tool that does not address the special needs of psoriasis [3]. Using this tool in 80 psoriasis patients, a Greek study showed that more than 88% of partners were affected by the disease and that their own hrQoL was impaired [9]. Similar data using the FDLQI were seen in a Spanish cohort of 130 participants [10].
Apart from the FamilyPso, only the Psoriasis Family Index (PFI) is specific for psoriasis [11]. However, only a refinement named PFI-14 is available but no data have been published using the tool [12]. The FamilyPso was developed to particularly cover emotional burden of partners. Apart from the study presented here the FamilyPso is used in a European multinational study which is currently ongoing [13].
Validating the questionnaire was a major aim of the FamilyPso international study. In addition, the burden to partners aged 18 years and above was assessed in six countries in parallel to prove its usefulness for cross-country/society comparisons. Demographic data of interest regarding patients and of their partners were captured.
The patients who were asked to complete the FamilyPso by their wife/husband or partner were middle-aged, with a long history of psoriasis and a high prevalence of psoriatic arthritis and comorbidity. As there were no inclusion or exclusion criteria for recruitment, this is an unselected cohort reflecting typical psoriasis patients presenting to outpatient dermatology practices or centers. Patients were asked to self-assess the severity of their current psoriasis, which was mostly mild, with 10.9% reporting severe disease, although there was wide variation between centers. More than 71% of patients were receiving treatment at the time of their assessment. We were able to show clear relationships between FamilyPso scores and self-rated psoriasis severity, which supports the validity of the instruments. Overall, the mean FamilyPso scores were found to be rather low. This may be due to the high rates of (presumably successfully) treated psoriasis in our samples. Depending on the rates of acute and severe psoriasis in a sample, mean FamilyPso scores may vary considerably. Further research and normative data are needed.
With the large sample of this investigation, we could validate the factorial structure of the FamilyPso by confirmatory factor analysis. The results implied a small modification for one item. In the original factor analysis, item 9 (stress caused by a partner’s pain and sleeping problems) had been part of domain B, “cleaning.” It is now part of domain C, “acute emotional strain,” showing improved face validity. The former result may be due the small original sample size, and to scaling in acute psoriasis, as acute illness causes stress and more cleaning. Except for this change, the structure of the five domains showed stability, their reliability was acceptable or better, and a total score was defined.
Weak measurement invariance was confirmed for gender and language. This means that the factor structure of the instrument is stable, while it can identify level differences between cultures or other discriminating subgroups. The measurement invariance for languages seems to indicate that the translation was successful and that the domains of the FamilyPso are common, with valid concepts across the cultures studied.
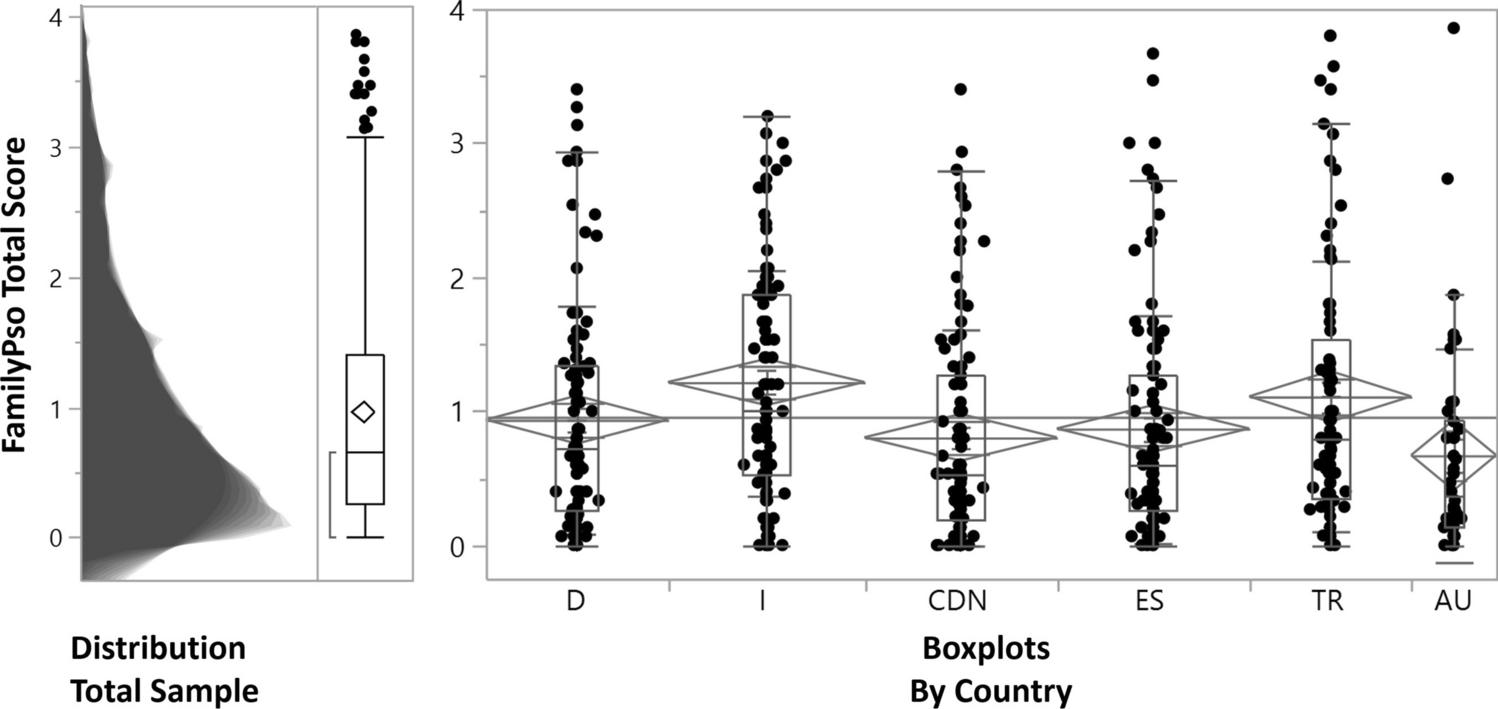
Item and domain statistics are now available from a large international sample, allowing comparisons and interpretation of score levels. Overall, the reliability of the FamilyPso has been validated and its use in further national and international research can be encouraged. On average, the FamilyPso total score showed low levels of partner distress across the study cohort. However, there was a clear dependency of burden and severity, with the highest being for the general emotional strain domain. This domain includes the items sympathy, making it my own problem, and feeling helplessness, which clearly describe the problem that chronic illness poses for partners. These findings are in line with data from a recent small qualitative study of 38 partners of psoriasis patients who reported in semi-structured interviews on emotional consequences such as embarrassment, frustration, helplessness, and pity [14]. Particularly wives and female partners had an increased score for the cleaning domain. This result is to be expected as women are generally more sensitive about cleanliness traditionally in many cultures, as women take the responsibility of cleaning their houses. Cleaning also adds to substantial out-of-pocket expenses that families may incur due to people having psoriasis [15].
There is data describing the impairment of the sexual life of patients, but also of partners [16, 17]. Sex life of partners is included in the domain acute emotional strain but the total score of this domain showed only a mild burden that may be explained by the majority having mild disease and being treated.
When comparing the data from the different centers the domains: social reaction, acute emotional strain, and social life had the highest scores in Italy compared with the other countries. This discrepancy is difficult to explain. Austria and Canada are among the top 15 countries in the recently published Global Happiness Report, while Italy is ranked 33rd. However, Spain is ranked 32nd and Turkey 106th, so there is no argument on a country-by-country basis regarding the happiness parameter (https://worldhappiness.report/ed/2023/).
The strengths of the FamilyPso international study are the wide coverage over countries from North America to Turkey, as well as the large number of people with psoriasis and their respective partners investigated. Some limitations of this study are that validation of the different language versions and a direct comparison with other instruments was not performed, and that the self-assessment of psoriasis severity by the patients may differ from a dermatologist’s objective assessment, and may be biased in relation to the partners’ perceived burden. However, self-assessment of psoriasis is more frequently used in web-based investigations [18]. Another limitation may be the restriction to partners above the age of 18 years; however, this was part of ethics approval. Addressing the burden of children of people with psoriasis living together with people with psoriasis may be the aim of future studies.
In conclusion, the data of the FamilyPso international study validated the FamilyPso questionnaire, induced minor modifications in the settings of the five domains, and provided a sound basis for its further use in clinical studies. Comparing the data from respondents over six countries it was shown that this instrument allows the comparisons of different populations regarding the burden to partners of people with psoriatic disease.






Comments (0)