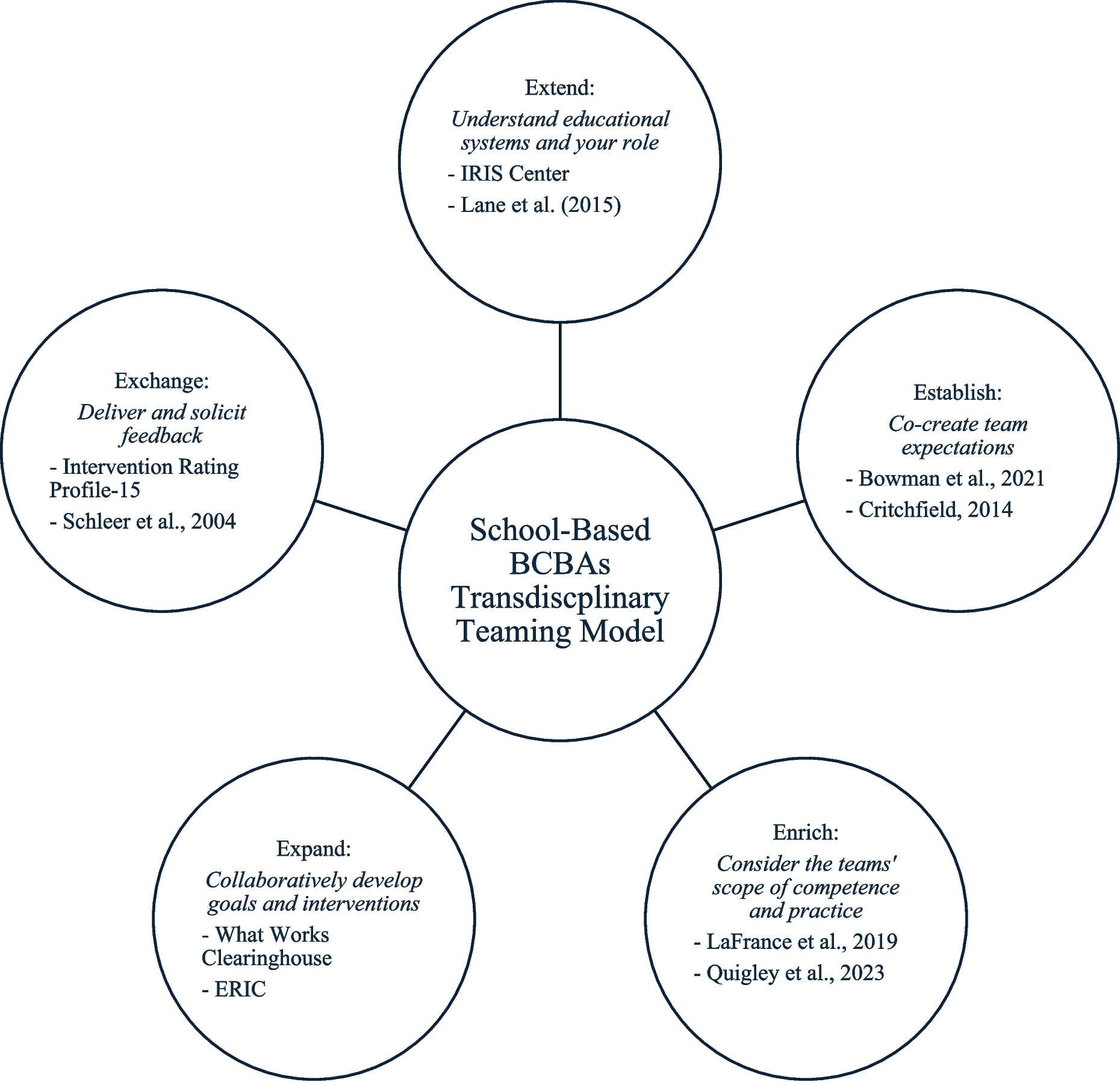
Figure 1 shows the group experiential theme and subthemes generated within this analysis across both case studies. Throughout this section, participant quotes are provided to support ideas generated in the analysis. Some quotes have been adjusted from original comments in the transcripts for brevity, signified by ellipses.
Clinical Practice is About Navigating the Continuum of Expertise
The group experiential theme developed in this analysis is that of successfully navigating the continuum of expertise. For both participants, navigating the continuum of ways of knowing (or holding expertise) within the intervention context was described as the central work of behavioral clinicians toward fostering interventions that fully involve parents. For participants, this continuum of expertise is present and pervasive in every clinical intervention context; that is, a part of all clinical interactions. However, having rich experiences on both sides of the expertise continuum helped to “bring into focus” or make evident this process of navigation, in ways that might be less visible or available to clinicians who do not hold dual roles as a clinician and a parent. For Anna and Mia, wearing two hats provided an opportunity to stand back and acknowledge the tensions that exist between different ways of knowing in a child-focused intervention context and how these can be successfully balanced throughout an intervention.
Within this global theme, focus on successfully navigating between both types of expertise (or ways of knowing) was described as a way to help parents feel engaged and connected and ensure they get what they need from interventions, while supporting clinicians to feel they are providing useful input to the families they are serving. The tensions and challenges of navigating this continuum of experience were borne out in a range of examples through participant recounting of experience. These include the subthemes: prioritize experience and knowledge, ask and don’t tell, meet parents where they are, and look for fit.
In this analysis, these subthemes present contexts/domains in which parents and clinicians navigate who holds power and agency within a collaborative child-focused intervention context.
Prioritize Experience and Knowledge
Fundamentally, for participants in this study, successfully navigating tensions within an intervention context starts with seeing (and valuing) the knowledge, experiences, ideas, and expertise parents bring to interventions. Necessarily, this requires shifting preoccupation with, or de-prioritizing, the experiences clinicians bring to a child-focused intervention. The process of navigating expertise was exemplified in the exploration of how much (and with what level of genuineness) parents’ lived experience informed the development of an intervention, over clinical judgment or experience. For Anna, each parent’s experience with their own child immediately positions them as experts in the intervention:
It’s about seeing that the parents have the most experience. I see a lot of clinicians who go in thinking they know everything, and it’s like, unless you’re a lived clinician then I feel like you can’t know … it’s about listening to those parents as experts. (Anna, Interview 1)
Mia described a need to step back and consider the whole picture, including where parent expertise lies, rather than leading with your own clinical ideas of what works:
Wearing two hats helped me to look at the bigger picture, not so much of ... what skills this child is lacking or what strategies need to be done to teach this skill, more … taking steps back and looking at the context: is this family well supported? Are they burned out? Do they have services in place to help them with respite? Are they sleeping? Everything, just checking everything. (Mia, Interview 2)
On the basis of their experiences holding dual roles in behavioral intervention, participants both explored the place for awareness (or paying attention) on the part of clinicians to better understand the relative expertise of all parties and more carefully navigate whose knowing is prioritized at each stage of an intervention. When clinicians come to identify their potential biases and assumptions around whose knowledge counts, they can deprioritize the specific clinical concerns and instead ask, “What can I offer these parents?” challenging inherent power dynamics.
Rather than coming into work with parents “knowing” what intervention was required, Mia described that “I would bring in ideas, offer some input, take perspective, step back” (Mia, Interview 1). In this way, prioritizing parent knowledge shifts the boundaries around interventions in ways that “push parent voice to the top” (Anna, Interview 2) and provide opportunities for parents to self-advocate, for example, by saying, “Sorry I disagree with you.” (Mia, Interview 1). For Anna, this prioritizing of parent experiences and knowledge manifests in giving parents space to say what they know and don’t know (or want to know):
If they want education, we will always talk about that. Or if they want, we talk a lot with wider family, because often it’s getting other family acceptance. So, I guess I’m always coming from that lens … we need families to be resilient enough to care for their own people, with the very limited funding and supports that they get. One way to do that is to make things as easy as possible in that family, to hear what they need. (Anna, Interview 2)
For both Anna and Mia, negotiation around whose experience “counts” involves a level of humility on the part of clinicians to offer parents what they need rather than, perhaps, what seems clinically indicated in order to “give them the confidence to keep going” (Mia, Interview 2). Prioritizing parent expertise, in this account, involves giving away (or negating) some of the inherent power held by clinicians to enable parents to determine change. Mia offers this perspective:
When you go to a family’s home and you over-focus on the challenges of the children, you make the parents feel even worse about themselves. Then they’re likely to avoid you or avoid the service. Because you are actually making them feel completely powerless … [Clinicians] will say that they’re disengaged but they are not empowering the parents to say what they need. (Mia, Interview 2)
Ask and Don’t Tell
Navigating the continuum of whose expertise matters is especially critical at the outset of intervention, when clinicians are attempting to build therapeutic relationships with parents to establish their involvement. Consistently, participants highlighted the need to “ask and don’t tell” with parents to build a working relationship and exemplify that parent knowledge holds capital in determining the intervention context.
For both participants, this begins with simply creating the conditions for listening. Anna reflected on the space of listening in being a “genuine human” and not pushing your expertise to the top.
It’s about listening to those parents. That would be my biggest advice: that clinicians really need to listen. I’m sure a lot of them go in with preconceived ideas … you can form a picture and it’s that bias. I like to go into that first meeting without really knowing anything and then just … hearing what they say. (Anna, Interview 1)
Additionally, Mia framed this process of developing connection as one of giving parents more time and space to share their context and not “rushing”: “Understanding things that are important to the family, before starting hands-on work with the child, it will make the service so much more effective” (Mia, Interview 1). Where this can fall down is when clinicians, motivated by other competing variables, rush the process of listening and building connection: “They [clinicians] come in thinking too much of the problem and how to fix it, instead of holding space for parents, to understand where they are coming from” (Mia, Interview 2). Anna noted that often, clinicians are in such a hurry to get things going they lean on assumptions as a shortcut to understanding a family’s context, rather than asking parents directly:
Clinicians need to wait until the assessment is done before they start making those assumptions. Because they come in immediately, and they look around the house, and they think, ‘Oh yeah, this is- this is what’s going on here.’ Everyone’s trying to look for that- they’re trying to sort out their assessment before they’ve actually fully done it. And I think that’s ... detrimental. It doesn’t honor parents. (Anna, Interview 2)
Participants both explored the necessity of suspending judgment based on what you read, are told, referral details, or first impressions. Building on their experience, participants shared that judgment (or closed-mindedness) can move the intervention toward one that legitimates clinical experience over the parent’s lived experience and limits the parent’s ability to acknowledge their understanding of their child and their child’s needs. By asking (rather than telling), clinicians can let parents dictate the narrative. Allowing parents to communicate their understandings and expertise without framing within a clinical lens avoids feelings of judgment on the part of parents by clinicians. Anna comments that “just being able to talk about the behavior, and also with no judgment” (Interview 1) helps to navigate the continuum of expertise by giving parents space to share. Further, Anna describes how clinicians need to be “thinking about which questions they are asking. When you start asking those questions about parenting, or, you know, parent characteristics, things ... that can be where we lose them, because families feel judged, straight away.” (Anna, Interview 2).
For both participants, “telling rather than asking” holds an inherent risk for eroding parent collaboration within interventions. Mia summarized the idea that telling parents what to do does not help in creating a collaborative intervention context, as it risks damaging trust:
Imagine these parents, they are already feeling like they’re failing their child... and I come in and tell them what they’re supposed to do? No. They know what they are supposed to do. But they’re not well enough to make any changes. They’re exhausted. And so, I don’t feel like it’s my place to go there and make them feel even worse about themselves. (Mia, Interview 2)
Instead, offering support rather than specific intervention tools or strategies at the outset is protective (“more of... giving them support and letting them know I understood” Mia, Interview 2). For Anna, this means “I’m giving advice to families, rather than telling them what to do … cause I don’t think that ever works” (Anna, Interview 2).
Mia reflected that in her experience, the process of asking parents, rather than telling them, involves a level of perspective taking on the part of the clinician:
A lot of clinicians lack perspective-taking. They don’t get the parent’s perspective. If the clinicians put time aside to build that rapport with the parents, to understand where they’re coming from and where they get stuck, if they shift the parent’s behavior, the parents will make changes for the child. (Mia, Interview 2)
Mia described this process as the building of trust, where over time and through repeated pairing, clinicians come to be viewed by parents as trustworthy and as holding genuine care for their child and their family, purely through prioritizing listening and nonjudgmental communication. In this way, asking parents (rather than telling parents) helps clinicians navigate the continuum of expertise such that strong, trusting relationships are developed within intervention contexts to support meaningful and ongoing parent involvement.
Meet Parents Where They Are (Frame Challenge and Opportunity)
Within child-focused behavior analytic interventions, navigating expertise—or whose way of knowing (e.g., identifying contingencies) carries more weight—is exemplified in the tensions between acknowledging the inherent challenges of parenting children with additional support needs and framing these challenges toward a more productive outlook. In this analysis, meeting parents where they are involves flexibility and humility on the part of the clinician to create a safe space for parents to express the difficulties inherent in their lived experience, while sensitively creating opportunities to see the potential and value of interventions for their child and family.
Participants described awareness and keen understanding of how challenging it can be for parents who are seeking supports for their child/ren, stemming from their own parenting experiences. For Anna, the experience of parenting a child with additional support needs is a “tough” one, framed as difficult or “hard”: “It’s hard, it’s demoralizing, you’ll hear that time and again from parents… you are fighting and its hard” (Anna, Interview 1). Anna explains that she sees parents as always in survival mode or in spaces where “the mental energy has gone on just coping” (Interview 2), informing parent perspectives and positioning interventions in the space of difficulty or challenge. For Mia, this experience is one of constant pressures and demands:
“You really feel lonely, you get frustrated, you feel like no one understands you. Eventually you just stop sharing and you isolate yourself” (Mia, Interview 1).
In the context of seeking support, the parent’s experience of the challenge is further exemplified:
“Having to run around and attend appointments, managing all that and having to chase professionals, doctors, support needs services, schedule therapy, it is non-stop! It is hard” (Mia, Interview 1).
In the realm of clinical work, both Mia and Anna describe the role a clinician can play in recognizing where parents are at in understanding or processing their unique situation while sensitively navigating between providing time for parents to express their feelings and creating opportunities for parents to view situations from a more optimistic lens. In explaining this balance, Mia described that parents “have to be in the right frame of mind” (Interview 2) in order to hold the emotional and practical challenges of their parenting journey together with the belief that things can improve and that there is benefit or “real hope” (Interview 2) in engaging with child-focused interventions. Anna explained that sharing her experience was a way to offer hope to some families for progress and change by recounting how she had lived through the struggle and grief:
Lived experience … is being able to give hope to parents that, yes, it is hard, but it changes. When parents can see that you’ve come out the other side, you know? Ok, he’s 14, we’ve managed this long, nobody’s died, that’s a good thing! That’s always reassuring, isn’t it? (Interview 1)
By contextualizing her own situation and how her thinking has changed over the years of parenting her son, Anna is able to offer this insight to families, to identify where they are positioned in understanding their situation, and to help them frame their experience in a way that balances difficulty with the potential for change afforded by intervention and supports. Similarly, for Mia, experiences as a parent allow her to share her learning with other parents in a way that validates what they are going through while providing an opportunity for optimism in intervention:
I [am] able to give them words of comfort, to help them process their grief and what they need to get through. The first thing I do is definitely acknowledge how tough it is. And if they give me any space to say anything I would suggest if they were open to ABA, I would also recommend that, so the conversation would really... be dependent on how open this parent was. (Mia, Interview 1)
Participants in this analysis caution that finding the balance between providing space for parents to express the challenge of their situation and prompting other ways of thinking is difficult. For Mia and Anna, this requires careful reflection on the part of the clinician to gauge where a family is positioned and decide the relative value of reframing this experience for involving parents in interventions and not “turning them off.” Anna describes this tension:
I will tailor what I say to a family and their individual circumstances. Definitely. There are some families who are still very much in the grief stage and don’t … want to hear about the positive sides. They do just want to focus on what’s going wrong, how horrible it is. And so, it’s ok to let them stay in that space for a while because the child they thought they were having and what they have is … sometimes very different. And it is hard for families, and they all grieve at different rates. But I’ve always seen it as a ‘Ok, this is what we’ve got. What do we do next?’ kind of thing. (Anna, Interview 2)
Look for Fit
For participants in this analysis, with experience on both sides of the expertise continuum, a key area where negotiation takes place is in positioning the intervention to fit the family context (while also aligning with the service delivery context). In this subtheme, tensions exist around clinicians letting go of power to decide and instead giving control to parents to imagine an intervention that matches their needs and resources.
Mia explains that this process begins by developing a fuller understanding of the learning histories and environmental variables relevant to each family and finding out what is possible for that family to achieve.
I usually sit down with the parents and I do a, a thorough check. I just, I ask. I ask: do you get respite? What services do you have in place? And then I pick up on what they need. And I let people know, that this family needs this and that. I’m happy to provide strategies, but families won’t be able to implement until they have those other things in place. So, I usually advocate for that first. (Mia, Interview 2)
For Anna, who was a parent before practicing behavioral interventions, acknowledging the parent’s limits and capacity (e.g., available resources) for doing so is essential to shaping what intervention is offered.
Actually, people don’t understand how hard the job is and 24/7 supervision is incredibly taxing. So, being able to just make little changes. Like, I’m not the clinician who goes in and writes a 10-page plan with ridiculous goals and strategies. Often, my goals look like, ‘We’re going to put in positive strategies that will implement quality of life for the person and their family.’ That’s generally it, and then we will put in- even using a first and then. Or helping with toilet training. Because if you could help with, just say toileting, and getting them so that they’re not doing washing every single day or spending hundreds of dollars on pull-ups and things, usually you find that other behaviors will decrease because you have put in some positive stuff. Small stuff.” (Anna, Interview 2)
Critically, recognizing variability in service delivery models and taking time to understand parent expectations around particular services is a way to avoid setting unrealistic or unfounded expectations and, ultimately, to make sure the intervention being offered is a practical fit for that family. For both participants, the breakdown in parent involvement and collaboration comes when clinicians “really push families” (Anna, Interview 1) and are inflexible in their expectations or delivery, leading parents to a place where: “they know what they are supposed to do. But they’re not well enough to make changes. They’re exhausted” (Mia, Interview 2). In this analysis, such inflexibility—or prioritizing clinical fit over parent and family fit—often means families pull away or refuse services, even if they want and need the support. Mia explains: “Parents push them away, it’s too hard, it’s too much. Too much pressure. The demand is too much. And I feel like a lot of clinicians don’t see that. They miss that point.” (Mia, Interview 2). Anna recounts that sometimes the way interventions are structured or delivered puts families in a space where: “parents just couldn’t … they don’t have capacity to do that” (Anna, Interview 2). For participants in this analysis, successful behavior analysis is about balancing the clinician’s impulse to know and decide with awareness of where families are at and what they can do: “I can see what I think would make a difference, but parents just don’t have capacity to do it. So, what’s the value?” (Anna, Interview 2).
Participants explored that sometimes, it is not about the intervention specifics, as much as getting the timing right and making space, for now to be “not the right time.” Anna explains:
When parents say to me, ‘Look, this is just not the right time,’ … that is exactly one of our options when we early terminate, not the right time. And that’s ok. Because if there’s huge family pressure and things happening … that will be contributing to behavior. But you’re still got to deal with that before you can deal with the behavior. And sometimes that, that’s the hardest thing [for parents], is realizing—and saying—that actually ‘now isn’t the right time.’ (Anna, Interview 1)
In order for clinicians to fully involve parents, sometimes they need to step back and consider if the personal resources available to families “match” what clinicians are offering or if they need to change what is offered. Mia describes awareness of parent positionality as determining how intense interventions can be: “I can’t expect a burnt-out mum to make changes when she can’t look after her own health. They have to be in the right frame of mind to implement anything” (Mia, Interview 2). Often, this means giving parents the agency and relative power or control over the situation to “choose to say yes” or to “choose to say no,” without the risk of being labeled as noncompliant or disengaged by clinicians (or necessarily contracting contingencies of punishment associated with discharge from services). For Anna, this is about supporting parents to develop their own agency to decide and to negotiate what is being offered in service of “helping” that child and family:
And it’s like, but... what if they can’t? Like that’s … it’s not that they won’t, it’s that they can’t. Because what you’ve decided to do, all the homework or the data collection that you want them to take, all of this is actually just not possible at the moment. So, what can you do to make that easier? (Anna, Interview 2)
Importantly, being flexible and responsive to parents’ needs and wants while recognizing that parents “can’t disengage from their child” (Mia, Interview 2) and can only choose to be more or less involved in each intervention setting will support clinicians to offer interventions that are a good fit for parents, promoting active involvement.



Comments (0)