This study shows that, in a real-world clinical setting with a nationwide implemented tumor-first testing workflow, approximately one out of three EOC patients did not receive the recommended BRCA1/2 testing. The overall percentage of patients who completed the test-pathway did significantly increase in the third and fourth year compared to the start, with 74.4% completing the test-pathway in the most recent year. Patients were also significantly more likely to complete the test-pathway if they were younger at diagnosis, diagnosed with high-grade serous/high-grade endometrioid carcinoma, diagnosed with stage III/IV, had high or middle SES, and had received chemotherapy or surgery.
A tumor testing workflow would, theoretically, result in greater equity with respect to access to DNA testing in comparison to former germline-based workflows. Significant improvements in testing rates were reported in patients with high-grade serous ovarian cancer after implementation of reflex BRCA1/2 tumor testing [18]. Furthermore, preliminary results of the nationwide implementation project showed that tumor tests were offered to more than 80% of all included patients [8]. Here, we took a rigorous patient-centered approach to evaluate full completion of the tumor-first test-pathway, and our evaluation shows that inequities in testing still remain. Clinical and patient characteristics independently influence the likelihood of completing the test-pathway, and these insights may be used to address barriers to testing, as outlined below.
First, a younger age and high-grade serous/high-grade endometrioid histotype were significantly associated with higher odds of completing the test-pathway. This finding may originate from the clinician’s perspectives that patients with these characteristics are more likely to carry a PV. Nevertheless, the mean age of diagnosis in BRCA2 carriers does not substantially differ from that in sporadic EOC diagnoses [19, 20]. Additionally, while we have previously shown that causal BRCA1/2 PVs were exclusively detected in high-grade serous/high-grade endometrioid carcinoma [17], selectively testing these tumors requires accurate histopathological diagnosis and possibly central pathology reviews, which is not structurally implemented before testing. To optimize identification of potential BRCA1/2 carriers in this patient population, it is advised to test all patients regardless of their age and histotype [7].
Next, patients with advanced-stage disease were significantly more likely to complete the test-pathway compared to those with early-stage disease. This could be driven by the PARP inhibitor indication being limited to patients with a PV in the tumor and advanced-stage disease in the first-line setting [21]. However, the tumor test is not solely implemented to determine PARP inhibitor sensitivity, but simultaneously determines potential genetic predisposition. Therefore, testing patients with early-stage disease remains essential to determine genetic predisposition and subsequently reduce cancer incidence and mortality among relatives of the patient.
Importantly, patients with high and middle SES were approximately two times more likely to complete the test-pathway compared to patients with low SES. Considering the pathology-based universal reflex testing and full reimbursement of tests, we anticipated the influence of SES on the likelihood of receiving the test to be limited. However, low SES has been linked to less aggressive treatment strategies and lower survival rates in ovarian cancer patients [22], which could explain the observed inequities. Regardless of SES, patients who received chemotherapy or surgery were more likely to complete the test-pathway compared to patients who did not receive chemotherapy or surgery. While chemotherapy and surgery are standard of care for patients with FIGO stage IIb-IV, 31% of the patients in our cohort did not receive chemotherapy and 31% did not receive surgery. Not receiving chemotherapy could indicate a rapidly progressing disease, where chemotherapy could not be timely provided or was not expected to provide benefits. Not receiving surgery limits the availability of tumor tissue required for the tumor test. DNA can also be isolated from ascites or tissue obtained by biopsies, but this could not be evaluated in the current study. It is essential that clinicians are aware of the need to refer patients for a germline test, even when prognosis is poor or tumor tissue is not available, as determining genetic predisposition can have lifesaving consequences for relatives.
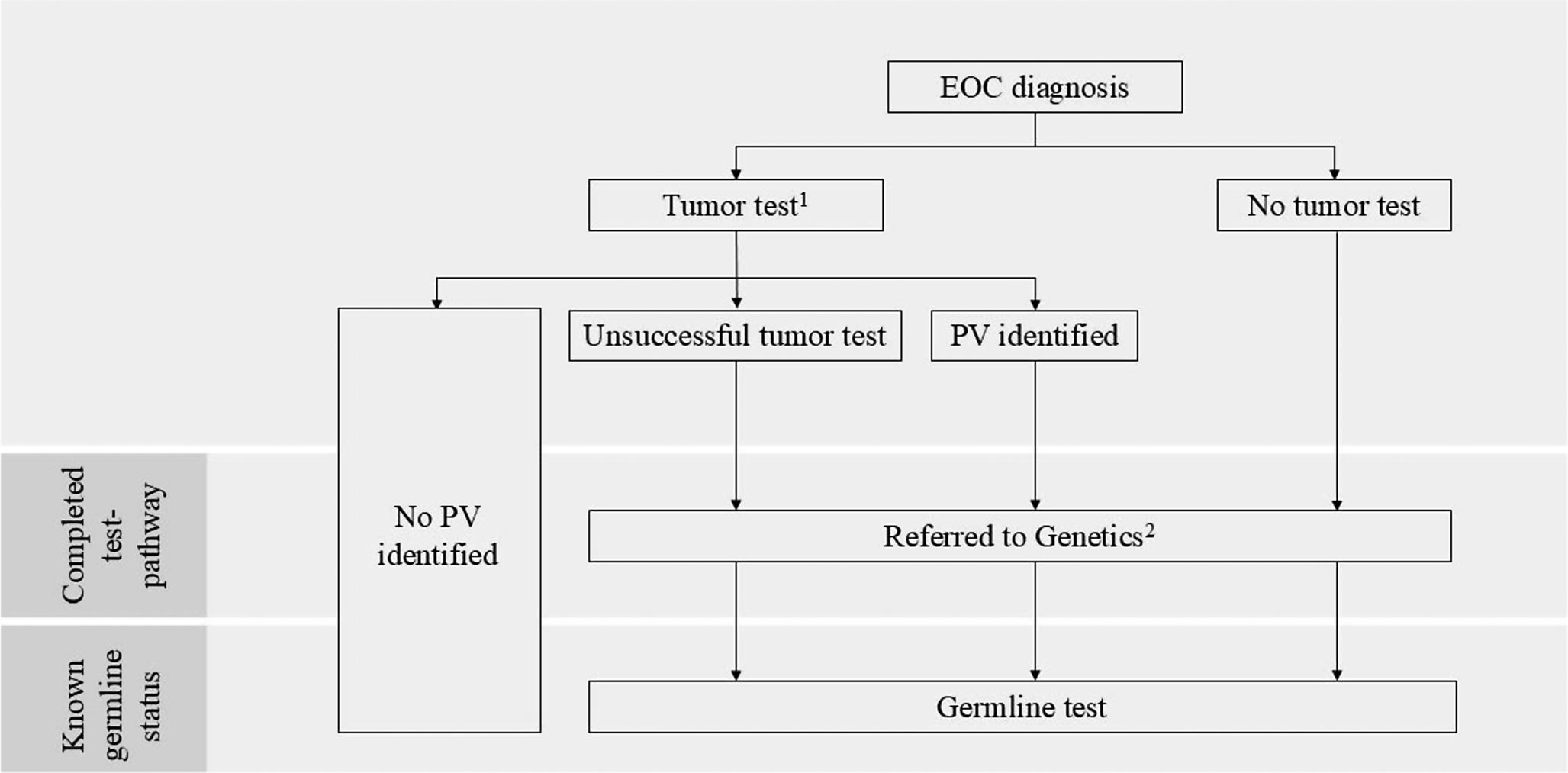
Not all patients with a positive tumor test and subsequent referral to clinical genetic services (i.e., completion of the test-pathway) actually proceeded with germline testing. Notably, patients may decline a germline test. Therefore, we decided to analyze the percentage of patients referred rather than tested, as this most accurately reflects the extent of adequate test-pathway implementation. In our series, a few patients passed away after referral and before the germline test, highlighting that lack of time due to poor prognosis potentially limits test-pathway completion. Implementing mainstream germline testing within the tumor-first pathway could accelerate the process of determining genetic predisposition and further increase test uptake [23]. This would be particularly valuable for patients with rapidly progressing disease and for the relatives of these patients. Under a mainstream germline testing pathway, pre-test genetic counseling and blood sampling would be provided by trained gynecologic oncologists as part of routine care. Post-test counseling with a clinical genetics service would be offered to those who carry a PV, as well as to patients without a PV, but with a relevant personal or family history (e.g., personal history of breast cancer, or personal/family history of Lynch syndrome-associated cancer). Nevertheless, the high morbidity and mortality of EOC patients complicate testing uptakes, emphasizing the need to adequately counsel relatives if the patient cannot be tested.
A limitation of this study is that we heavily relied on reported data in patient files. While it is not expected that patients were genetically tested without this being reported, it is unknown to what extent tests performed outside of our regions, relocation of patients, declining a test, or testing of family members, are being reported in patient files. Our estimates are, therefore, a real-world reflection of what is reported in patient files but could underestimate the actual uptake. Regional hospitals were contacted to obtain additional information on untested patients. Moreover, we acknowledge that a tumor- rather than germline-based testing approach is not endorsed by all countries. Yet, our study approach and the identified patient populations that were less likely to be tested are informative and likely applicable to other (germline-based) testing approaches.
In conclusion, approximately one out of three EOC patients was not offered BRCA1/2 testing. This study highlights the need for better adherence to current guidelines, particularly in older patients, those with low SES, low-grade histotypes, early-stage disease and those who do not undergo surgery or chemotherapy. Additionally, timely DNA testing, and testing relatives if testing the patient is not an option are crucial to increase testing rates. Ultimately, this will enhance care for patients and reduce the incidence and mortality of cancer in relatives with a hereditary predisposition for EOC.





Comments (0)