We report current research training practices, supports, and productivity among nearly 75% of pediatric cardiology training programs in the USA. Our study identified a misalignment between ACGME requirements, research training resources and practices, and workforce trends. Essentially all programs have mandatory clinical and academic responsibilities during research time, and many fellows pursue additional elective clinical time during these weeks. Research resources are limited at many programs, including inadequate faculty mentorship and lack of funding support. Most program directors thought that the current 12-month research requirement should be shortened and replaced with an individual curriculum tailored to the needs of each trainee.
Our data provide the first description of the current national implementation of research requirements in pediatric cardiology fellowship programs. The vast majority of programs meet but do not exceed the requirement with exactly 12 months of research in their curriculum. Research months are more common in the second and third years of fellowship, consistent with a heavy clinical workload during the first year in most programs. The large portion of time allotted to research, including half of the third year, is in contrast to the 3% of practicing pediatric cardiologists who report spending more than half of their time on research [4]. The varied and increasing clinical settings in which fellows require training (cardiac critical care, echocardiography, interventional cardiology, electrophysiology, etc.) has increased pressure on the 24 months of clinical training during fellowship. Fellows seek out additional clinical experiences to further their mastery of clinical cardiology and to better prepare themselves for the workforce. This is consistent with the fact that most fellows now pursue additional and advanced subspecialty clinical training, mostly through fourth-year fellowships [3]. The increase in fourth-year training is driven in part by the increasing complexity within these clinical disciplines. Additionally, much of the research time currently incorporated into fellowship is in the second and third years of training. Significant research time late in the third year may lead to a lack of clinical exposure immediately prior to the transition to the attending role, leaving fellows underprepared for this transition if entering practice after three years.
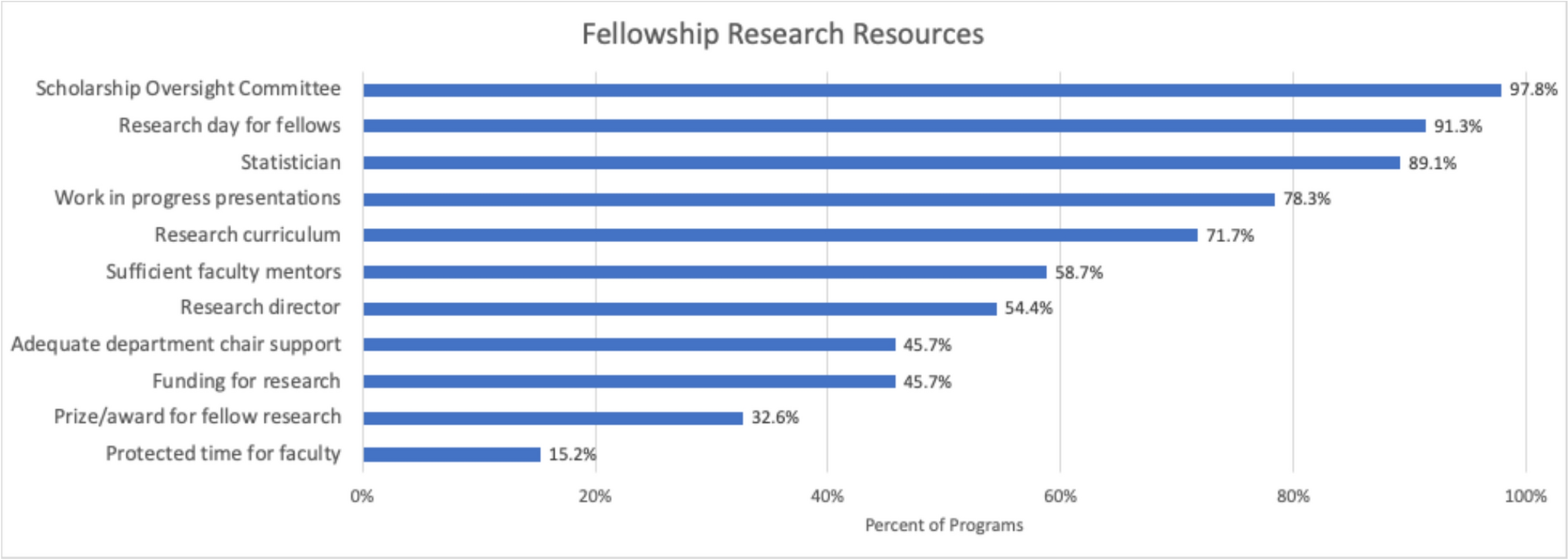
There were significant gaps in resources available to support fellow research. Nearly 30% of programs reported not having a structured research curriculum despite this being an ABP requirement for board certification [2], as well as correlated with increased productivity without increasing the amount of research time [9, 10]. Additionally, there are notable deficits in faculty and financial support of fellow research. Although research mentorship has been found to be an important factor in research productivity both in pediatric residencies [11] and fellowships [12], more than 40% of programs report insufficient faculty mentorship, and only seven programs report protected time for faculty to provide mentorship. Finally, fewer than half of programs reported funding for fellow research. Accrediting bodies should consider formal criteria for the support for fellow research afforded by programs and institutions.
Our findings are consistent with a recent survey of pediatric cardiology fellows [13]. This study found that just 31% of fellows were satisfied with the research methodological training they have received in fellowship. Like our study, they identified lack of protected time for faculty to support fellow research, lack of formal research training, and lack of funding for fellow research as key barriers. Interestingly, they identified that 26% of fellows reported having nine months or less of protected research time. This contrasts with the 4% of program directors in our survey, although these numbers are not directly comparable as multiple fellows could have been from the same program. This survey of fellows did not directly address whether fellows would prefer shorter research requirements.
Most fellowship program directors thought the current 12-month research requirement should be shortened, and most did not think this would affect the overall productivity of scholarly activity or the community of physician scientists. This is aligned with the preference of most fellows who indicate they would shorten their fellowship by shortening the research requirements if the option were available [6]. Interestingly, there is no ACGME research time requirement for adult cardiology fellowships [14]. Although not formally analyzed in this study, the desire for shorter research requirements was echoed by written comments in the survey. It was generally thought that if the research requirement were shortened, those interested in research could utilize additional elective opportunities to expand their work, while those not interested in research could seek out other opportunities relevant to their clinical goals. Many were in favor of tracks within programs that would allow research- or clinically focused fellows to pursue different allocations of their training time. Such changes would be in line with the recent update to the ACGME pediatric residency requirements, which emphasize flexibility and individualization [5]. Additional rotations individualized to the trainee’s goals may allow some fellows to acquire advanced clinical skills and experience during their three-year categorical fellowship that would normally require a fourth-year fellowship. Further, the increasing clinical complexity in pediatric cardiology, together with the recent ACGME changes to pediatric residency, have substantially increased the challenge of providing adequate training within the clinical training portion of fellowship. With changes in residency training, incoming fellows will have less inpatient clinical experience and some of that training will now need to occur in fellowship. Importantly, physicians across specialties show limited ability to assess their competency [15]. While many fellows express a desire to shorten fellowship by decreasing research time [6], using this for additional elective clinical or research time based on interest may provide more robust training.
Limitations
We are limited in part by the potential for response bias, including that those who are satisfied with current research requirements may be less likely to respond. The effect of this on the findings is likely minimal given the relatively high response rate. As in all survey research, there is also the potential for social desirability bias. It is possible that available resources are more limited than reported. Finally, we report the responses of program directors and not fellows themselves. It is possible that fellows may report different preferences regarding protected research time and the desired length of the research requirement. This is an interesting area for potential research. Further, program directors who are new to their role or have limited direct engagement with fellows may not fully understand the impact of research training on the fellowship experience.


Comments (0)