
Remember me

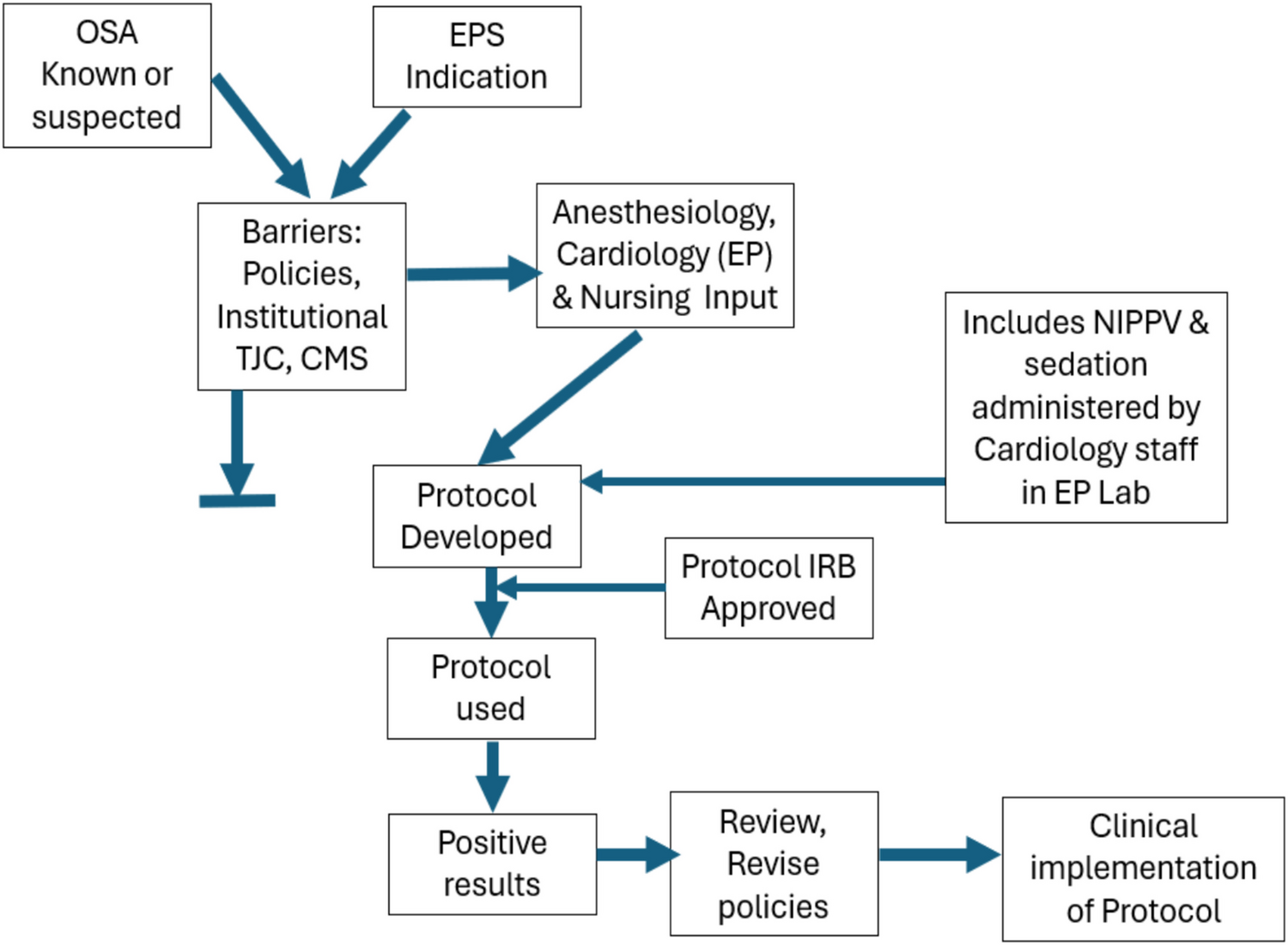
The protocol was approved by the Montefiore-Einstein Institutional Review Board for the Protection of Human Subjects (IRB), and all patients were fully informed and signed the IRB-approved consent form. We proposed that a pilot study be done with 20 patients to evaluate the feasibility of NIPPV during their EPS procedure. After the initial 20 patients, the IRB recommended increasing the study to 50 patients, without any protocol changes. The process is summarized in the central illustration (Fig. 1).
Fig. 1
Central illustration. This flow chart depicts the themes and progression of this protocol for the use of NIPPV with sedation administered by cardiology staff in the electrophysiology laboratory/procedure room. Barriers, particularly (obsolete) policies needed to be overcome. The IRB-approved protocol deferred barrier policies, and the positive outcomes led to a review and likely revision of related institutional policies
2.1 Personnel and processTraining of the nurses was confidence-based and was provided by the Department of Respiratory Therapy in conjunction with the Anesthesia Department to assure that the electrophysiology nursing staff were competent and comfortable with the use of the NIPPV machines. During training, each nurse was proctored by a respiratory therapist, and patients were not included in the present study if the nurse was still in the proctoring process. All nurses and physicians passed a certification process including ACLS and education in deep sedation, which included a video module developed and updated by one of the authors (VJ, a senior anesthesiologist). Many nurses had prior CCU/ICU experience, but this was not a pre-requisite.
The training included how to properly apply the mask on patients, titrate the FiO2/oxygen flows, and adjust the mask as needed based on the patient’s needs via simulation and didactic training. Physicians were instructed on the physiology and function of the NIPPV and titration of the parameters and sedation via didactic training by the respiratory therapists. Rather than pre-set flows or doses, continual titration aimed achieving and maintaining target patient responses. Fire prevention and responses [23] were stressed. These, together with respiratory therapy and anesthesia teaching processes, as well as the study protocol formed the syllabus for training.
2.2 Inclusion and exclusion criteria2.2.1 Inclusion criteriaMale or females aged 18 years or older with ≥ 1 of (1) diagnosis of OSA by sleep study; (2) history of observed apnea by bed partner; (3) neck circumference > 18 inches for males or > 16.5 inches for females; (4) patients with BMI > 27.
2.2.2 Exclusion criteria(1) Patients known not to tolerate a CPAP or BiPAP mask; (2) patients not able to give written or verbal consent; (3) patients who did not wish to participate in the NIPPV study. Prior use of nocturnal CPAP or BiPAP at home was not a criterion for inclusion or exclusion. Patients with unstable arrhythmias (the essence of most EP studies) were not automatically excluded.
2.3 Related policies deferred for this protocol by the IRBInstitutional policies were reviewed, with Montefiore-Einstein as an example [16, 17]. These policies call for arterial blood gas (ABG) analysis at 30 min during NIPPV procedures. This is not current practice in most EP, gastroenterology (GI), or other procedures. Policies exclude unstable arrhythmias. However, such arrhythmias are the essence of most EP studies.
Restraints are excluded during NIPPV. The positioning straps used in our laboratory procedure rooms were questioned as possibly fitting the CMS or TJC definition of restraints [18,19,20], and we proceeded to explore this through legal counsel and queries to TJC and CMS. Ultimately, it was determined that TJC and CMS regulations indicate that “positioning” devices used during procedures are distinct from restraints and are permitted [18,19,20]. See the Discussion section.
Finally, policies excluded sedation plus NIPPV outside of settings such as the various intensive care units. However, EP procedures are performed in cardiology procedure laboratories, not in intensive care units.
2.4 Sequence2.4.1 RecruitmentAt their pre-procedure visit, patients who fit the profile of a possible sleep apnea patient were invited to participate in the NIPPV study. Informed and signed consent was obtained in agreeing patients. One objective was to estimate the ability of non-anesthesiologists to select patients who met inclusion criteria and who could safely undergo NIPPV. Therefore, anesthesia consultation was not used routinely prior to the procedure. Anesthesia services are widely available at our institution, but only 2 of 50 participating patients had a pre-procedural anesthesia consultation. All patients underwent institutionally standardized pre-procedure evaluations including ASA and Mallampati-equivalent assessments separately by both nursing staff and cardiology physicians,
2.4.2 In the EP laboratoryPatients were brought to the EP lab, and once positioned on the EP table, they were continuously monitored by an ACLS-certified nurse experienced in the use of medications given for moderate/deep procedural sedation. All current EP laboratory registered nursing staff are experienced in catheterization/EP laboratory critical care, as per above.
The patients were assisted with the placement of a NIPPV mask. Oxygen was administered at a sufficient flow rate to bring oxygen saturation (SpO2) to 95–98% while the patient was awake; this was designated as the baseline SpO2. Arterial lines and blood gases were not used. After an initial period of 5–10 min of spontaneous breathing on oxygen, BiPAP was applied at a setting of 10 cm H2O IPAP and 5 cm H2O EPAP achieved gradually over 5 min. If nasal airflow did not achieve near-baseline levels, further increases in IPAP and EPAP were instituted in 2 cm H2O increments every 5–10 min.
Baseline measurements of heart rate, respiratory rate, chest wall motion (CWM), SpO2, and respiratory airflow (Vi) were recorded for 30 s. Then, IV sedation/analgesia was administered and titrated as per our usual protocol [3] to attain a level of sedation that would allow the patient to remain comfortable on the EP table for the duration of the procedure. The sedation target was usually “moderate” but could vary from light/minimal to brief periods of deep sedation, e.g., during implantable defibrillator shock testing.
Medications given for sedation/analgesia in our EP laboratory include midazolam, fentanyl, morphine, and diphenhydramine. Agents, such as propofol and ketamine, cannot be administered by nurses in non-intubated patients in New York State (21). Reversal agents, naloxone and flumazenil, were immediately available.
Non-invasive blood pressure measurements were taken every 5 min; pulse oximetry (SpO2), heart rate, and end-tidal carbon dioxide (PETCO2/ETCO) were monitored continuously, with appropriate alarms, and chest wall movement (CWM) was monitored by observation and/or auscultation. Each EP laboratory is equipped with a defibrillator and a bag valve mask if there was a need for increased ventilation. High-flow nasal prongs were available. A kit for intubation was readily available. Respiratory therapy and anesthesiology backup were available.
The physiologic data was displayed in 30-s epochs, and obstructive apneas were identified by comparison of chest wall motion and air/O2 flow (Vi) and quantified as to frequency and duration. Episodes of respiratory distress or desaturation (< 88% SpO2) were identified and quantified for each subject.
If at any time during the EP procedure, the patient’s SpO2 approached 80% for longer than 1 min despite appropriate routine interventions (listed in the next sentence), the EP procedure was suspended, and the NIPPV mask was removed. Such patients were mask-ventilated with the continuation of verbal stimulation, cessation of additional sedation, head tilt, or jaw lift maneuvers until the SpO2 was greater than 92%. Procedure failure occurred if the SPO2 could not be raised to ≥ 92%. If the oxygen saturation could be raised above 92% and stable, then at the discretion of the cardiologist, the EP procedure was either terminated (protocol failure) or continued with or without NIPPV in place until the end of the EP procedure (always without if SPO2 fell to ≤ 80% for ≥ 1 min). Similarly, waveform capnography/PETCO2 was followed, and continuation of the procedure was assessed if the waveform changed or PETCO2 dropped to 15–20 mmHg, depending on baseline and rapidity of change and whether up-titration of ventilation restored PETCO2 to ≥ 35 mmHg.
Recovery followed current guidelines, which include monitoring the patient in an appropriately staffed and equipped area until they were at or near their baseline level of consciousness and were no longer at sedation-related increased risk for cardiorespiratory depression. Oxygenation, ECG, and blood pressure were monitored.
The risks involved with this study were expected to be the same as risks associated with giving moderate/deep procedural sedation and the same as risks that are involved with a standard EP procedure in OSA patients. These risks include, but are not limited to, nausea, vomiting, aspiration, apnea, hypoxia, hypercapnia, possible need for endotracheal intubation, and arrhythmias that could require defibrillation. If any of the above-mentioned adverse events occurred, clinical discretion was used to determine whether the EP study would or would not be completed. It should be noted that induction of arrhythmias is often part of an EP study. Therefore, intentional induction of arrhythmias was not considered as a complication.
Data collected for the purposes of this study but not as selection-inclusion criteria included the following:
1.Patient demographics, such as gender and age, and clinical data, including BMI, neck circumference, type of procedure, length of procedure, and American Society of Anesthesiology (ASA) class (I–VI). In view of known or suspected OSA for the patients in this study, all were assigned a minimum of ASA class II.
Airway assessment: In lieu of the widely used Mallampati score (class 1–4), Montefiore developed an institution-wide pre-anesthesia sedation system. This involves separate forms for physicians (EP cardiologists for this report) and nurses. Points are often redundant for quality and confirmation purposes; both include anesthesia-sedation history and airway assessment, together with the ability to lie flat, dental condition, mouth opening, neck extendability, obesity, and OSA history. A Mallampati equivalent score (MES) was used in the present report, with 0–2 classes added for each abnormality depending on severity. For consistency, all MESs were assigned by one investigator (JDF) and subsequently reviewed by at least 1 other investigator during the manuscript preparation process.
2.Physiologic data included intra- or post-procedural episodes of hypoxia or respiratory distress, O2 saturation ranges for each patient (baseline and with NIPPV), PETCO2, need for reversal agents, and time to restoration of O2 saturation ≥ 92% after a desaturation event.
3.Clinical data: procedure time, completion or cancellation of procedure, and sedation medications.
4.Patient toleration was defined as completing the procedure with NIPPV.
2.5 ConfidentialityAll information collected for this study was considered private in accordance with HIPPA guidelines. While the results of the research study may be published in a scientific journal, all patient identifiers were removed. Patients agreed to this use of data as part of the informed consent process. Protocol, IRB approval, and individual data for each patient are available.
The main outcome measures were safety (the number of NIPPV-associated complications) and efficacy (the number of procedures completed vs. those that had to be canceled or interrupted because of respiratory difficulties).
Regarding safety, for this study, we expected no NIPPV-associated complications causing an adverse outcome.
Regarding efficacy, the purpose of the study is to improve the ability to perform EP studies in sleep apnea patients unassisted by anesthesiology or respiratory therapy, but with rapid backup available. Patients who did not sufficiently maintain their oxygenation status, or regain a SPO2 > 92 despite using NIPPV while receiving sedation/analgesia, were considered a failure for the purposes of this study. The IRB predefined a failure rate of 25% to be acceptable.
2.6 Statistical analysisAs indicated in the Methods section, this was a study of 50 consecutive consenting patients with known or at high risk for OSA who agreed to receive sedation for their EPS under the direction of an electrophysiologist. No attempt was made to select for type or number of procedures, gender, procedure time, or other factors. Statistics and analysis were limited to (1) safety: whether the procedure was safely completed from a NIPPV perspective [11, 13,14,15]; (2) efficacy: actual use of NIPPV and delivering desired levels of sedation; (3) descriptive matters such as patient and procedure details; and (4) a review of local and national guidance documents.
Comments (0)