The study protocol was approved by the Clinical Research Ethics Committee of Erciyes University (2019/280, 17 April 2019) and was supported by the Scientific Research Project Group of Erciyes University (TSA-2020-10085).
Informed consent was obtained from the patients’ parents. Upper gastrointestinal endoscopy (using a Fujinon 4400-HD-EG530FP model endoscopy system) was performed on pediatric patients presenting with dyspeptic symptoms to the Erciyes University Faculty of Medicine, Department of Pediatric Gastroenterology. Male and female patients aged 6–18 y with untreated dyspeptic complaints who underwent upper gastrointestinal endoscopy and biopsies were taken from the antrum of the stomach were included in the study, while patients with endoscopy indications other than gastritis were excluded from the study. During endoscopy, four biopsy samples were taken from the antrum, two for histopathological examination by the pathology department and two for bacteriological and molecular analysis, which were stored at -80 °C in the Department of Microbiology of the Faculty of Veterinary Medicine of Erciyes University.
Biopsy samples stored in Brain Heart Infusion Broth (CM1135, Thermo Fisher Scientific, USA) were homogenized using a sterile glass pestle. After incubation, colonies suspected to be H. pylori were analyzed for phenotypic tests (Gram stain, morphology, motility, catalase, oxidase and urease activities) [6].
DNA was isolated from both the H. pylori isolates (from culture-based and from the gastric biopsy samples) using the EasyPure® Genomic DNA Kit (EE101-12, TransGen, China) according to the manufacturer’s instructions.
Species-specific PCR amplifying the phosphoglucosamine mutase gene (glmM) was used to confirm H. pylori isolates identified by phenotypic testing and to detect H. pylori in gastric biopsy samples [7]. PCR products were analyzed by 1.5% agarose gel electrophoresis (Biomax, Agarose, lot number 124543PR, Prona, European Economic Community) and visualized under a UV transilluminator (GChemi XRQ; Syngene, Cambridge, UK). Bands of 294 bp were considered positive for H. pylori.
Each of the ten virulence genes of H. pylori was analyzed with a single PCR. The amplified products were electrophoresed on a 1.5% agarose gel, and product sizes of 271 bp, 349 bp, 508 bp, 247 bp, 229 bp, 567/642 bp, 259/286 bp, 190 bp, 187 bp and 213 bp were considered positive for babA2, cagA, cagE, iceA1, iceA2, vacA m1/m2, s1/s2, s1a, s1b and s1c, respectively [8,9,10].
Genotyping was performed using the Enterobacterial Repetitive Intergenic Consensus-Polymerase Chain Reaction (ERIC-PCR), as described by Versalovic et al. [11]. Primers 1R and 2 were used for PCR. Electrophoresis of the amplified products was performed on a 2% agarose gel. The banding patterns of ERIC-PCR were analyzed using BioNumerics software version 7.6 (AppliedMaths, Ghent, Belgium). The similarities between strains were calculated using the Dice coefficient and a dendrogram was generated using the Unweighted Pair Group Method with the Arithmetic Average (UPGMA) clustering algorithm. A similarity index of > 80% was used to define clusters [12].
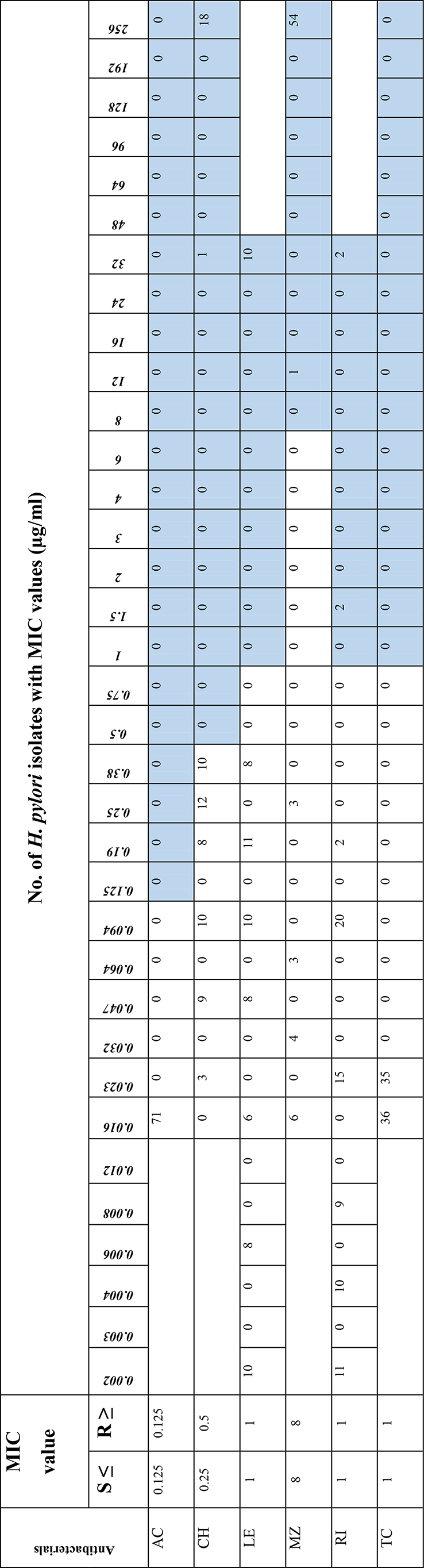
The gradient method was used to determine the antibiotic susceptibility of 71 H. pylori isolates from biopsy samples. The antibiotics tested included amoxicillin (AC), clarithromycin (CH), levofloxacin (LE), metronidazole (MZ), rifampicin (RI) and tetracycline (TC) (Biomerieux, France). The minimum inhibitory concentration (MIC) values were interpreted according to the limits given in the EUCAST guidelines [13]. The MIC values (mg/L) of amoxicillin, clarithromycin, tetracycline, metronidazole, levofloxacin, and rifampicin were ≤ 0.125, ≤ 0.5, ≤ 1, ≤8, ≤ 1, and ≤ 1, respectively.
The Helicobacter pylori ATCC 700824 strain was used as the reference strain for the culture-based examination and molecular analysis.
The gastric biopsies were fixed with 10% formalin and tissue processing was performed using the Leica ASP300 tissue processor according to the standard protocol for tissue processing in authors’ pathology department. From the paraffin-embedded blocks, 5 μm thick tissue sections were cut with a microtome and mounted on standard slides for hematoxylin-eosin staining and on polylysine L-coated slides for immunohistochemical staining. Immunohistochemical staining was performed on the Ventana Benchmark Autostainer with the polyclonal antibody against rabbit H. pylori (Zeta Corporation, Arcadia, CA, USA) at a dilution of 1/200.
Gastric biopsies stained with hematoxylin-eosin were examined under a light microscope using the updated Sydney system for the presence of H. pylori, chronic and active inflammation, intestinal metaplasia and atrophy. Immunostaining was performed by a single pathologist for the presence of H. pylori. Brown staining in the sections was considered positive, indicating the presence of H. pylori. The pathologist was blinded to the PCR or culture results.
Statistical analysis was performed using IBM SPSS v.26. Descriptive statistics for numeric variables were reported as mean and standard deviation or median and interquartile range. Categorical variables were presented as frequencies and percentages. The chi-square test was used to assess the relationships or differences between categorical variables. The normal distribution of the data was assessed using hypothesis tests and graphical methods (Shapiro-Wilk test, histograms, QQ plots, etc.). For comparisons between two groups, a t-test for independent samples was used if the assumptions of normality were met; otherwise, the Mann-Whitney U test was used. A significance level of p < 0.05 was considered statistically significant.





Comments (0)