Study design and population
We studied etanercept-naive participants with RA who initiated ETA-B or ETA-O between January 2015 and May 2022 from the cohorts contributing to CAN-AIM’s biosimilars registry. We restricted our analyses to participants with at least one follow-up visit following etanercept initiation and sufficient data to calculate disease activity and remission.
Data sources
We included data from four prospective cohorts in Alberta and Quebec: (1) the RA Pharmacovigilance Program and Outcomes Research in Therapeutics (RAPPORT) initiative, a prospective cohort registry in the province of Alberta (Edmonton and Calgary) collecting data since 2004; (2) the RHUMADATA® registry, an observational clinical practice registry collecting data on RA patients of the Centre de l’ostéoporose et de rhumatologie de Québec (Quebec City, Quebec [QC]) and the Institut de rhumatologie de Montréal (Montreal, QC); (3) the Early Undifferentiated PolyArthritis (EUPA) cohort, a registry collecting data on individuals diagnosed with early inflammatory arthritis at the Centre hospitalier universitaire de Sherbrooke (Sherbrooke, QC); and (4) The Université de Sherbrooke Registry of Advanced Therapies (USRAT), a registry of patients prescribed at least one advanced therapy by a rheumatologist from the Centre intégré universitaire de santé et de services sociaux de l’Estrie-Centre hospitalier de Sherbrooke (CIUSSS de l’Estrie-CHUS) since 2003 (Sherbrooke, QC)[9,10,11]. This study received approval from the McGill University Health Centre Research Ethics Board (MP-37-2019-4560) and complies with the Declaration of Helsinki. The research ethics boards of the participating institutions reviewed and approved the study protocol. Participants provided written informed consent.
Variables
Exposure was defined as the use of ETA-B (Brenzys™, Samsung Bioepis Co., Ltd.; Erelzi®, Sandoz Inc.) or ETA-O (Enbrel®, Amgen Inc.). The index date was defined as first-time exposure. Outcomes of interest were remission and sustained remission. Disease remission was determined based on the disease activity scales available in each registry. For the RAPPORT, EUPA and USRAT registries, we used the Disease Activity Score 28 (DAS28)-CRP, Clinical Disease Activity Index (CDAI), and Simplified Disease Activity Index (SDAI). The RHUMADATA® registry, on the other hand, exclusively collected data on DAS28-ESR and SDAI. Remission was defined as DAS28-CRP or -ESR < 2.6, SDAI ≤ 3.3, or CDAI ≤ 2.8 [12,13,14]. These scores are validated and widely accepted methods for assessing RA remission, with evidence demonstrating a good correlation and comparability among them [15]. Sustained remission was defined as at least two consecutive visits in remission within the first 12 months of follow-up among participants with a minimum of 12 months of follow-up.
We used baseline characteristics (at index date) to characterize the population and adjust in multivariate analyses. We included biological sex (female versus male), race (White versus non-White), age at RA diagnosis (years), age at ETA initiation (years), mean RA duration (years), mean body mass index (BMI), obesity (BMI ≥ 30 kg/m2), calendar year (> 2017), current smoking status, disease activity (SDAI score as continuous variables; and as moderate or high disease activity, based on ≥ 1 of the following: DAS-28-CRP/ESR ≥ 3.2; CDAI > 10; and/or SDAI > 11), past use of other bDMARDs, and concomitant prednisone, methotrexate, or hydroxychloroquine use.
Statistical analysis
We described cohort characteristics using absolute numbers (n) and proportions (%) for categorical variables and mean with standard deviation (SD) for continuous variables. Additionally, we calculated the difference in proportions and means between ETA-B and ETA-O initiators’ characteristics, with 95% confidence intervals (CI) calculated using the Newcombe-Wilson score method and Wilcoxon testing.
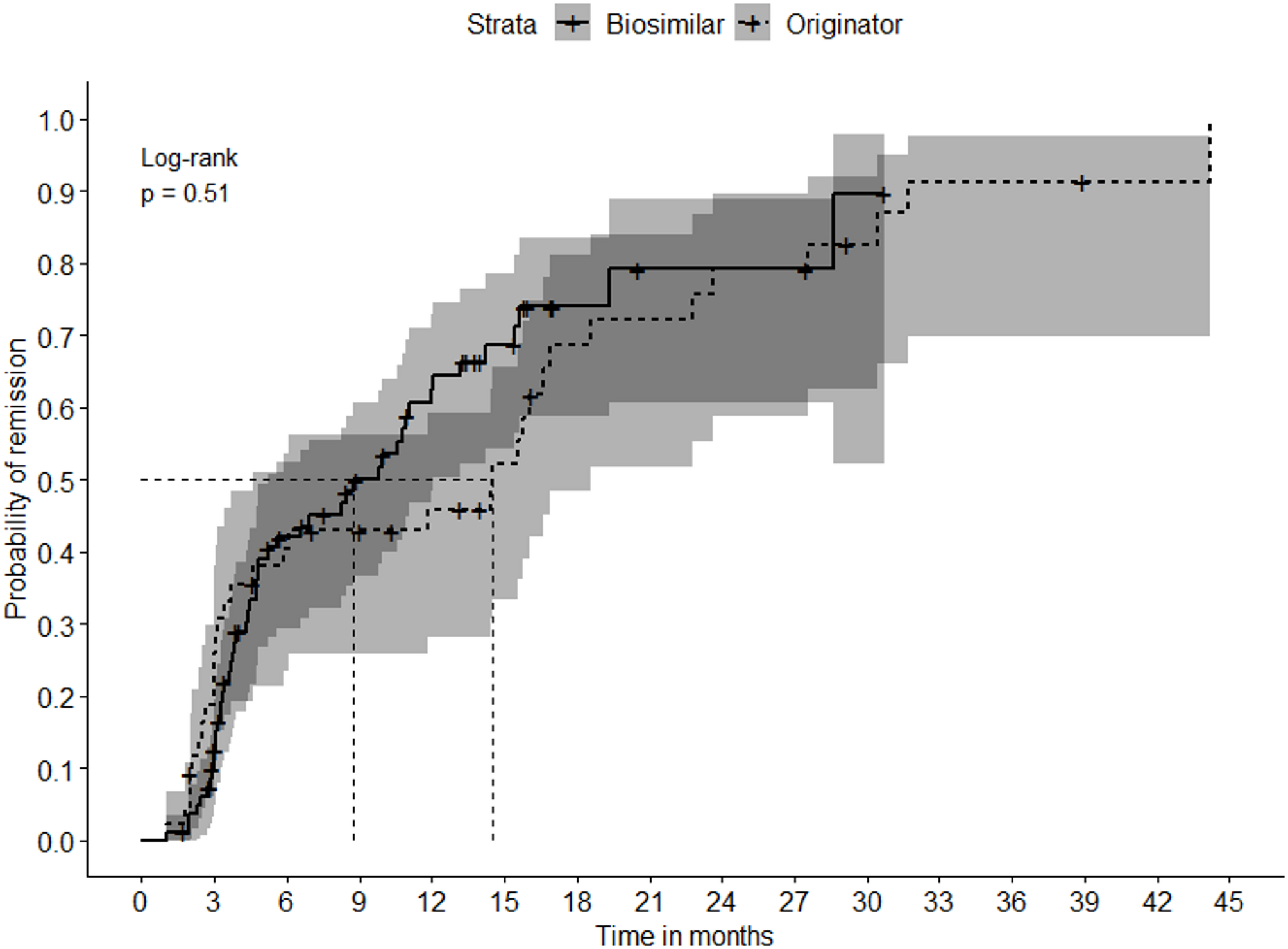
For the remission analysis, we selected participants with active disease (i.e., not in remission) at ETA initiation. We used Kaplan-Meier curves to calculate the median time to first remission, accounting for censoring due to treatment discontinuation (e.g., intolerance, insufficient disease control), loss to follow-up (e.g., patient transfer, relocation), or death, whichever came first. The log-rank test was performed to compare time to first remission between the groups. We conducted multivariate Cox proportional hazards regression to compare the probability of remission between ETA-B versus ETA-O, presenting the results as hazard ratio (HR), unadjusted and adjusted (aHR). Logistic regression was used to assess sustained remission, expressed as odds ratio (OR), unadjusted and adjusted (aOR). As mentioned earlier, we adjusted for potential effect modifiers and confounders (i.e., biological sex, age at RA diagnosis, RA duration, BMI ≥ 30 kg/m2, current smoker status, moderate or high disease activity, concomitant methotrexate, hydroxychloroquine, and prednisone use). The proportional hazards assumption for the Cox regression model was assessed using Schoenfeld’s test [16], while the goodness-of-fit of the logistic regression model was evaluated using the Hosmer and Lemeshow test [17]. We assessed statistical significance using 95% CI. For the log-rank test, we considered P < 0.05 as statistically significant. We used the R software for the analyses.



Comments (0)