
Remember me


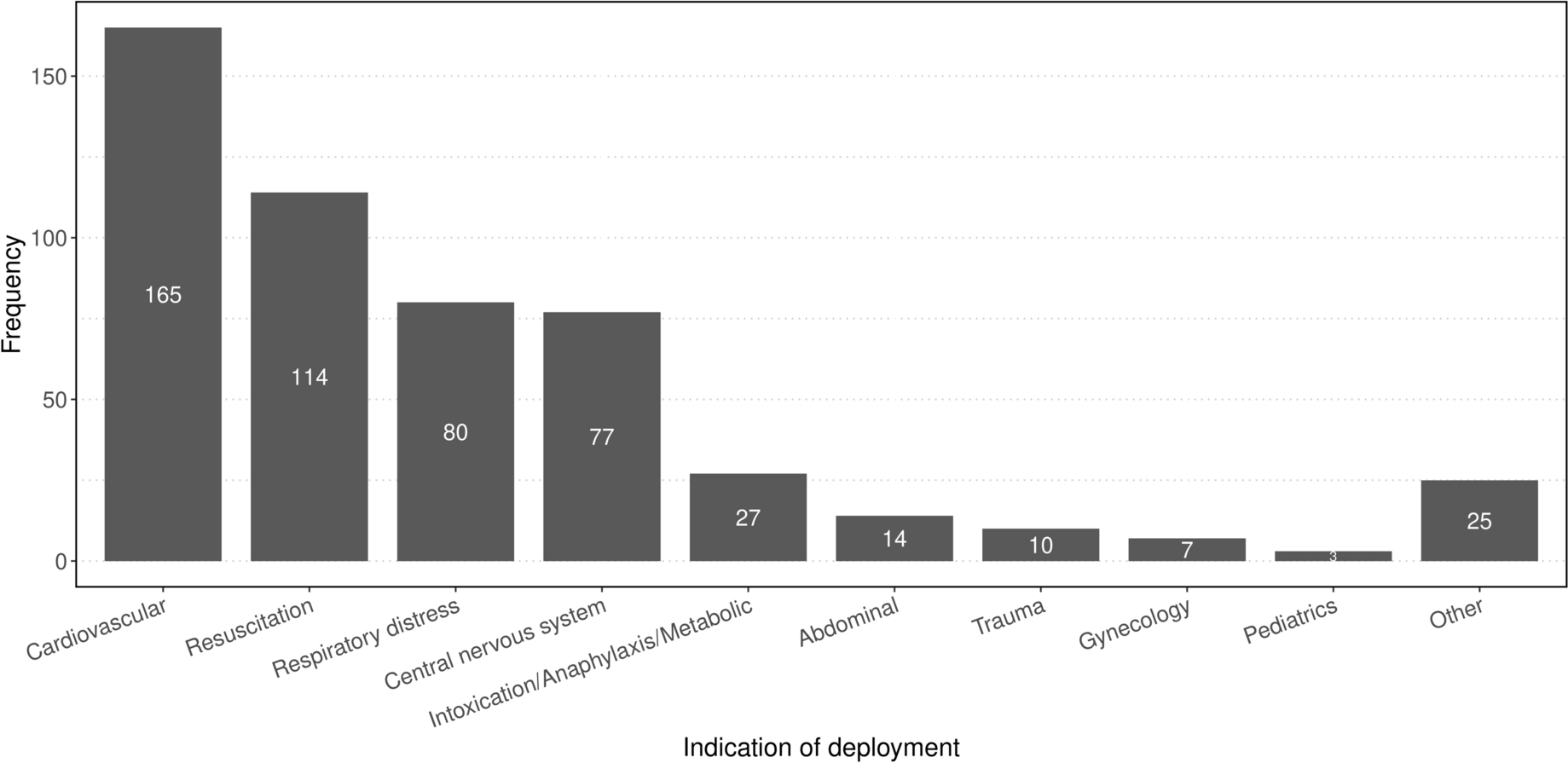
During the observation period, the MET was deployed 522 times, averaging approximately 0.36 deployments per day. A total of 53.2% male (n = 278) and 46% female patients (n = 240) and patients’ unknown sex (0,8%, n = 4) were treated; the median age was 66 years. The most common indication for deployment were cardiovascular problems at 32% (n = 165), followed by resuscitations at 22% (n = 114) and respiratory distress at 15% (n = 80). Pediatric cases were very rare, accounting for only 0.5% (n = 3), but were always severe with a NACA-Score above 4. Although the MET is not routinely deployed to the pediatric clinic during daytime hours, it may be called upon at night in cases of resuscitation or anticipated difficult airways, additionally, the MET may encounter emergencies of pediatric patients in the functional suites (Fig. 1).
Fig. 1
Emergencies took place on general wards in 42.6% (n = 222) of cases, in 29.6% (n = 154) in the public area, 16.1% (n = 84) in functional suites, 4.4% (n = 23) in intermediate care units and 7.3% (n = 38) in intensive care units. In one case, the location was not documented. Life-threatening situations, defined by a NACA-Score of 5 or higher, within public places were exceedingly rare (1.3%). On general wards, a wide range of conditions was observed. In intensive care units the cases presented to the MET ranged from help with unexpected difficult airway to intra-hospital cardiac arrest. The serious pre-emergency status of the ICU patients contributed to the overall patient outcome of cases presented to the MET. On IMCs and in the functional suites, there was a more heterogeneous distribution of the NACA-Score, although the patients were more compromised compared to those in the public area but less than in the ICU as expected. Overall, an increase in the NACA-Score could be observed from the public area, through the general ward, up to the intensive care unit (Suppl. Figure 1).
Examining the NACA-Score in relation to the time of alarm, a clustering of critical emergencies was observed at night and on weekends. During the early shift, 17% of patients had a NACA-Score of 5 to 6 points. This proportion increased to 36% during the late shift and remained high at 38% during the night shift on weekdays. A significant imbalance was also observed on weekends; during the weekend day shift, 29% of patients had a NACA-Score between 5 and 6 points, and this proportion rose to 43% during the late/night shift on weekends. Furthermore, it was observed that the proportion of patients who were declared deceased either upon arrival of the MET or after CPR efforts remained unsuccessful (NACA-Score 7) also increased depending on the time of day. During the early shift on weekdays, 5% of all treated patients were declared dead at arrival, while this number increased to 12% at night and 18% during the night shift on weekends (Fig. 2).
Fig. 2
NACA-score distribution by shift
Emergency medication, invasive procedures and CPRThe need for interventions varied by site of incident. Emergency administration of medications was required in 85% of all emergencies during deployments to the ICU and in 89% of cases on the IMC. On the general ward, pharmacological therapy was needed in approximately 62% of cases, very similar to the functional suites where emergency medication was used in approximately 60% of cases. In contrast, it was indicated in only 16% in public areas. (Fig. 3). Overall, medication was authorized in nearly 50% (260/522) of all cases analyzed. Across all 522 interventions, intravenous vasopressors (adrenaline, noradrenaline, Akrinor®) were the most common pharmacological therapy used 151 times in 132 distinct emergencies. Endotracheal intubation was the most frequently performed invasive procedure in the examined cases, which had to be performed in a total of 136 cases (26% of all emergency responses). While 87% (n = 33) of the 38 patients in the ICU required intubation by the MET, it was necessary for 50% (n = 74) of patients on the general ward, and only 0.7% (n = 1) of the 154 patients in the public area (Suppl. Figure 2). Apart from oral intubations, other invasive measures were very rare; throughout the observation period, the MET performed a total of 3 cricothyrotomies and placed 5 chest drains. A difficult airway was documented in 27 intubations, accounting for 19.9% of all intubations. Consistent with the recorded NACA-Scores, the frequency of resuscitations also varied by location of emergency. In the public area, there was only one case of CPR, while the frequency of CPR was 14.3% (n = 12) in the functional suites, 44.7% (n = 17) in ICU, 33% (n = 8) in the intermediate care unit and 34.2% (n = 76) on the general ward. Among these, 62 out of 114 patients achieved ROSC, corresponding to a rate of 54.4%.
Fig. 3
Pharmacological therapy by location
Treatment resultsIn cases with a NACA score below 4, 87% (n = 134) of all patients in public areas underwent further evaluation in the emergency department, while 7% (n = 11) were discharged directly home. Admission to the operating room or the intensive care unit was rare in this setting, occurring in only 6% of cases (n = 9). Patients treated in the general ward were admitted to the ICU in 47% of cases (n = 104), with 19% (n = 42) dying before or during the deployment of the MET. Only 27% (n = 60) of the patients were able to remain on the ward and 7% (n = 42) were transferred to functional suites. Of patients treated in the ICU, 84,2% (n = 32) remained, 13,2% (n = 5) were declared dead, and only one patient, representing 2,6%, was immediately transferred to the OR.
Time of deploymentOverall, it is evident that the duration of deployments increases with a higher NACA-Score. While most cases with a NACA-Score of 1–2 were resolved within 30 min, the deployment time increases dramatically in more severe emergencies. In cases of resuscitation or patient death on the ward, the proportion of deployments lasting at least 30 min is considerably higher, accounting for 75% (n = 61) of all deployments with a NACA-Score of 6 and 67% (n = 57) with a NACA-Score of 7 (Fig. 4). There is a significant positive rank correlation of 0.566 (95%-CI [0.505–0.622], p < 0.001) between the NACA score and the duration of MET deployments, indicating that higher severity of patient conditions is associated with longer intervention times. Figure 5 demonstrates that more severe emergencies with higher NACA-Scores (5 to 7) predominantly occur during late and night shifts, regardless of whether they happen on weekdays or weekends. This trend is particularly pronounced for critical conditions, such as resuscitations (NACA 6) and deceased patients (NACA 7), where the probabilities are significantly higher during late shifts and night shifts, OR = 2.259 (95%-CI [1.597–3.190], p < 0.001). On weekends, the overall distribution of NACA-Scores shifts towards higher severity levels, with severe emergencies being more frequent compared to weekdays, OR = 1.831 (95%-CI [1.298–2.583], p = 0.001). Despite this imbalance, the difference between day and late/night shifts remains consistent, with severe cases being slightly higher during night hours, OR = 1.525 (95%-CI [0.858–2.710], p = 0.150). The model confirms statistically significant effects of shift timing (OR = 3.349, 95%-CI [2.287–4.924], p < 0.001) and weekends (OR = 2.713, 95%-CI [1.690–4.374]), as well as their interaction (OR = 0.455, 95%-CI [0.228–0.903], p = 0.025), providing critical insights for optimizing resource allocation and staffing during high-risk periods (Table 1; Fig. 5).
Fig. 4
Time of deployment according to NACA-score
Fig. 5
Estimated probability of NACA levels by shift and day type (Weekday vs. Weekend)
Table 1 Estimated probabilities [%] for NACA levels based on ordinal regression given day and shift of incident with corresponding 95% confidence intervals
Comments (0)