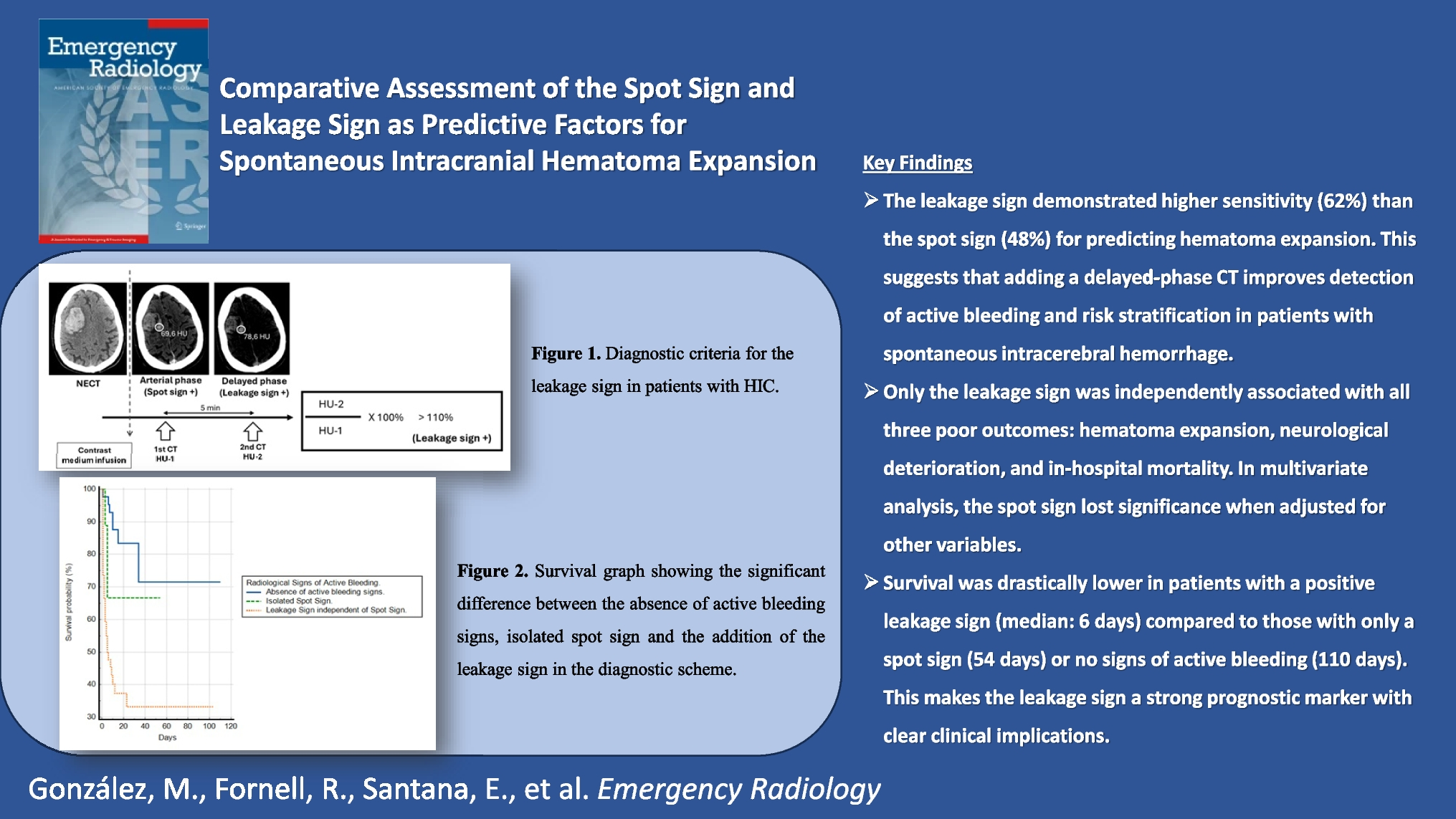
This study aimed to analyze the utility of the spot sign and leakage sign as predictors of spontaneous intracerebral hematoma expansion. The spot sign has traditionally been recognized as a radiological marker that, after contrast administration, helps predict active bleeding within intracerebral hematomas. For instance, Wada et al. first described the spot sign in 2007 as a radiological feature capable of predicting active bleeding in cerebral hematomas [3, 18]. Later, in 2016, Orito et al. proposed the leakage sign as a variant for the same purpose, arguing that its addition increases sensitivity and specificity when combined with the spot sign, without introducing technical complications [16].
The leakage sign is relatively easy to identify and only requires a delayed imaging phase following contrast administration. This additional phase improves sensitivity and specificity for predicting hematoma growth. One of the limitations of the spot sign is that normal or abnormal vascular structures may be misinterpreted as points of active bleeding. The leakage sign can help differentiate these situations: if a leakage sign is negative in the presence of a positive spot sign, it is possible to rule out active bleeding and instead attribute the finding to a vascular structure [19,20,21].
A potential drawback of the leakage sign is the need for patients to remain in the CT room longer, which may pose a risk for patients with clinical instability and rapid deterioration. However, in our series, no patients experienced cardiorespiratory problems or other signs that would contraindicate the 5-min wait between contrast injection and image acquisition. Orito et al. [16] also reported waiting 5 min before performing the delayed-phase CT for the leakage sign, obtaining sensitivity (93.3% (95% CI: 0.757–0.988)) and specificity (88.9% (95% CI: 0.815–0.912)) values similar to those found in this study.
Multiple authors agree that sensitivity and specificity for predicting hematoma expansion are enhanced when there is a longer time interval between the non-contrast CT (NECT) and contrast-enhanced CT (CECT) [16, 20, 22, 23]. Rather than relying on the leakage sign, some studies have employed multiphase CTA protocols with more than two phases and varying time intervals between each phase. For instance, in a study on spot sign detection using multiphase CTA, David et al. [22] demonstrated that the likelihood of detecting contrast extravasation in patients with acute spontaneous intracerebral hemorrhage increased with later imaging phases. Specifically, they reported contrast extravasation in 29.3% of patients in the first phase (arterial), 43.1% in a second phase (4 s delayed), and 46.3% in a third phase (15 s delayed). The use of a two-phase protocol with a longer time interval, as in our study, reduces the possibility of technical confusion during the imaging process.
In contrast to previous studies based on multiphase CTA, which have focused on the spot sign, few publications describe a clear protocol for determining leakage sign positivity. In our study, we provided an objective and reproducible method for determining leakage sign positivity by introducing a percentage increase in attenuation (measured in Hounsfield units) in the delayed phase compared to the early phase after contrast administration.
Few studies have explored the relationship between the spot or leakage signs and neurological deterioration or mortality, focusing more on their association with hematoma expansion itself. In the series by Takwa et al. [24], 30% of the cohort showed hematoma expansion, which was associated with worse neurological outcomes (lower Glasgow Coma Scale and NIHSS scores) and a higher in-hospital mortality rate (53.6%) compared to those without hematoma expansion (6.3%). Similarly, a meta-analysis by Davis et al. [25] found that for every 10% increase in hematoma volume, there was a 5% increase in the risk of death and a 16% increase in the likelihood of a worse outcome on the modified Rankin Scale, as well as an 18% increase in the probability of transitioning from independent function to assisted living or poor performance on the Barthel Index.
Beyond its prognostic value, the leakage sign may have important clinical implications in the acute management of ICH. Its presence could prompt closer clinical and radiological monitoring, including repeat neuroimaging within 6–24 h or earlier neurosurgical consultation. In settings where expansion risk is high, the leakage sign could influence decisions regarding intensive care unit (ICU) admission, escalation of medical therapy (e.g., blood pressure management or reversal of anticoagulation), and even consideration of surgical interventions such as hematoma evacuation or decompressive craniectomy. While further research is needed to validate the impact of leakage sign–guided management strategies on outcomes, its high predictive value supports its integration into clinical decision-making pathways for high-risk ICH patients.
Notably, in our study, the spot sign and the leakage sign demonstrated comparable sensitivity and specificity for predicting early neurological deterioration. This contrasts with their respective performance in forecasting hematoma expansion and mortality, where the leakage sign consistently showed superior predictive accuracy. One possible explanation is that neurological worsening in acute ICH is multifactorial and not solely driven by hematoma growth. Factors such as baseline hematoma volume, location (e.g., thalamic or brainstem involvement), intraventricular extension, and systemic variables including age, anticoagulant use, and preexisting brain atrophy can all contribute to clinical decline. As a result, radiologic indicators of ongoing bleeding may not fully capture the pathophysiological complexity underlying neurological deterioration. Similar findings have been reported in prior studies, which demonstrated that predictors of hematoma expansion did not always align with clinical outcomes in the acute phase [26, 27]. These results emphasize the importance of combining imaging biomarkers with validated clinical scales to more accurately assess early neurological prognosis in patients with ICH.
Beyond its prognostic value, the leakage sign may also carry significant clinical implications in the acute management of ICH. Its early detection on initial imaging enables timely risk stratification and may justify a more proactive clinical approach. In practice, its presence could prompt intensive monitoring strategies, including closer neurological observation, repeat neuroimaging within 6–24 h, or expedited neurosurgical evaluation. Moreover, in patients at high risk of hematoma expansion, the leakage sign might influence key management decisions, such as admission to intensive care units, aggressive blood pressure control, or early reversal of anticoagulation. In selected cases, it could also support the indication for early surgical interventions, including hematoma evacuation or decompressive craniectomy. Although clinical protocols directly incorporating the leakage sign as a criterion for such interventions have yet to be standardized, Orito et al. [16] emphasized its high predictive value for hematoma expansion. Additionally, Morotti et al. [19], in their recent meta-analysis, proposed that the combined assessment of the spot and leakage signs improves prognostic accuracy and helps identify patients who may benefit from tailored therapeutic strategies. These findings underscore the potential of the leakage sign not only as a radiological marker of poor outcome but also as a tool to guide early, risk-adapted therapeutic interventions in high-risk ICH patients. Nonetheless, prospective studies are still needed to validate its impact on clinical outcomes and treatment efficacy.
Limitations
Our study has several limitations. First, the implementation of a new protocol for this prospective study may have initially introduced technical difficulties in imaging or candidate selection. This issue was addressed through training of the involved professionals, ultimately resulting in a sample that met the established criteria. Second, the addition of a late-phase CT scan to the protocol increases the radiation dose received by the patient. However, this was validated by our hospital’s ethics committee, which deemed the potential clinical benefits outweighed the risks of additional radiation, especially for patients with potentially severe neurological conditions. In our series, the increase in radiation dose per patient was 670 DLP (dose-length product). Third, image review was performed in consensus by two radiologists. Future research should assess inter-observer variability through comparative studies.
Additionally, as this was a prospective study with a novel methodology not previously implemented in our hospital, there were instances where the on-call radiologists had no prior experience in performing or interpreting these studies. Nevertheless, the acquisition protocol was saved on the CT system for consistent use in all patients, and prior to the study's initiation, all on-call radiologists underwent basic training (2 h) conducted by two experienced neuroradiologists.








Comments (0)