
Remember me
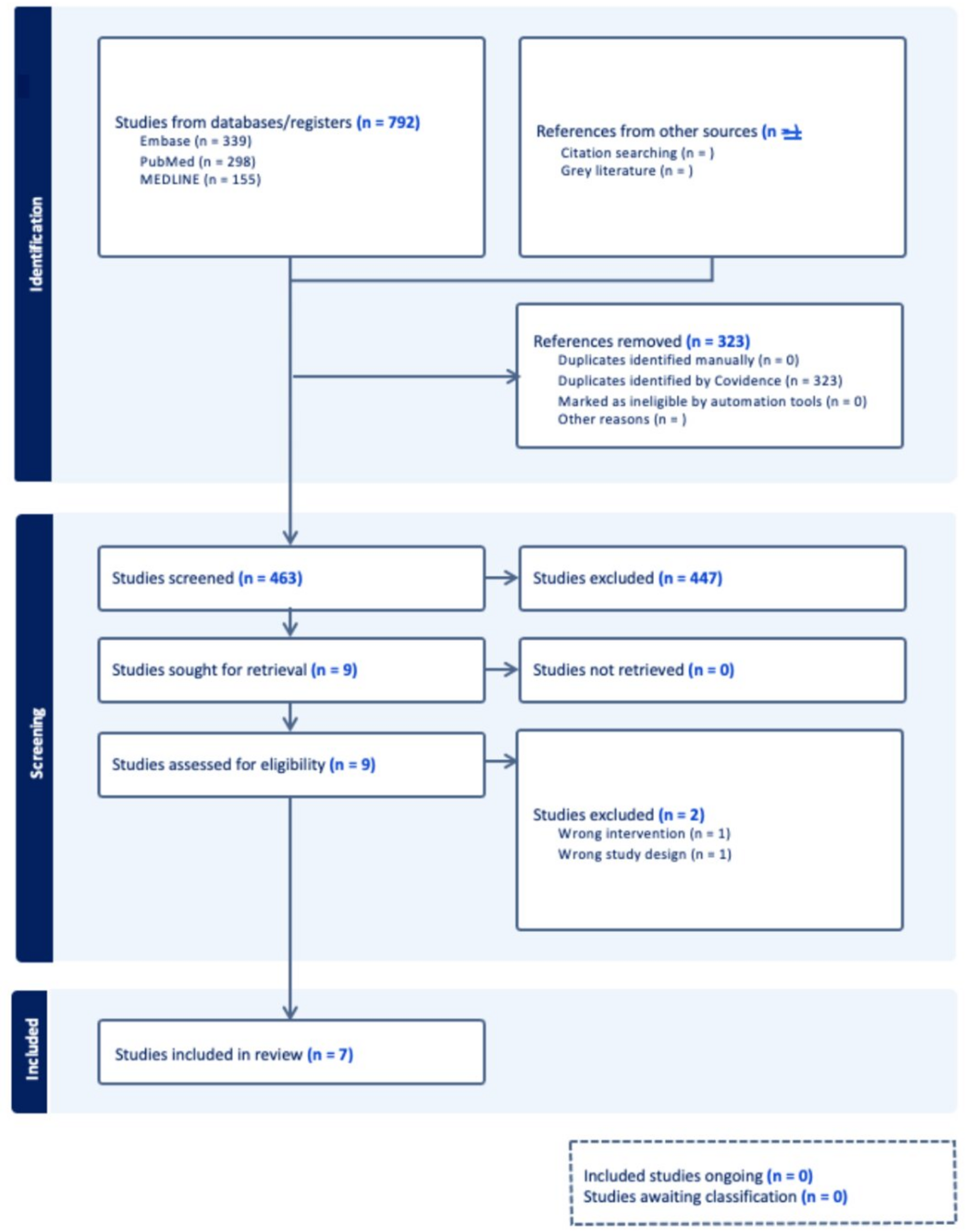





When assessing a patient with lower extremity deformity, initial evaluation involves obtaining a weight-bearing full-length mechanical axis view radiograph of the lower extremities to visualize the hip, knee, and ankle in the coronal plane for deformity analysis (Fig. 1), in addition to other views as needed (weight bearing anteroposterior, posteroanterior flexion, lateral, and Merchant views of the knee, or lateral tibial standing X-ray if evaluating for tibial slope).
Fig. 1
Full-length anteroposterior mechanical axis view and a knee lateral radiograph of a 25-year-old patient with right knee in varus alignment with excessive tibial slope, with a history of ACL reconstruction with allograft and meniscal repair, complicated by graft rupture, ACL tunnel bone grafting and osteochondral allograft to his medial femoral condyle, revision ACL reconstruction with hamstring autograft, and a subsequent re-rupture
Historically, osteotomies for the lower extremity were planned using only 2D radiographs [19]. However, variables such as flexion, limb rotation, and weight bearing have been reported to cause inaccuracies when using 2D imaging to plan deformity correction, especially when more than one plane may be involved [12, 20,21,22,23].
Volumetric imaging of the lower extremity, knee joint, or at least the proximal tibia if a multiplanar osteotomy is planned, is then obtained. The foundation of PSI in knee osteotomies is 3D volumetric imaging, such as CT or MRI. Some surgeons prefer CT scans over MRI because they are less expensive, have shorter acquisition times, can often be scheduled more quickly, and provide better resolution of bony anatomy [24]. While the downside of CT is ionizing radiation, modern, effective radiation doses can be reduced to the equivalent of one full-leg standing radiograph using low-dose scanning protocols and comes with the potential benefit of less fluoroscopy needed intra-operatively [24].
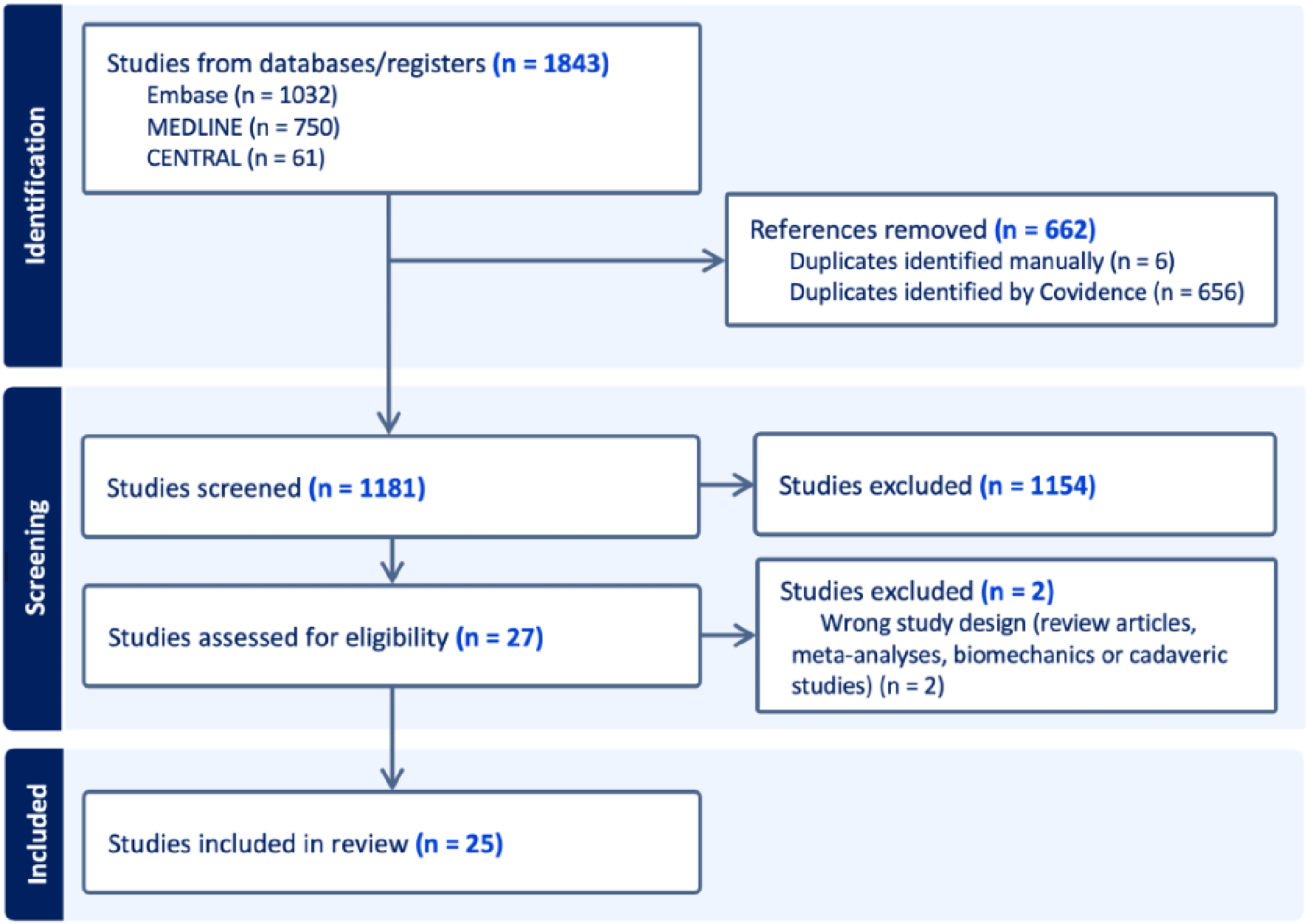
The 3D imaging files are then loaded into a software package for segmentation to create bone models and analyzed by 3-D planning software to create virtual pre-operative plans determining correction sizes and planned bone cuts approved by the surgeon [25, 26] (Fig. 2). The pre-operative templating software typically determines the exact length of each guide pin or screw, as well as plate size and shape, and can even take into account bone loss from the kerf of the saw blade [24]. 3D bone models, custom guides, and/or custom plates are made available to the surgeon intra-operatively to enable safe, efficient, and accurate plan execution (Fig. 3).
Fig. 2
The patient from Fig. 1 was templated to correct (a) varus with a femoral closing angle of 5.0° and gap of 5.1 mm with a lateral closing wedge distal femoral osteotomy with lateral fixation, and (b) a tibial slope correction of 10.7° and 10.7 mm with an anterior closing wedge high tibial osteotomy with medial fixation
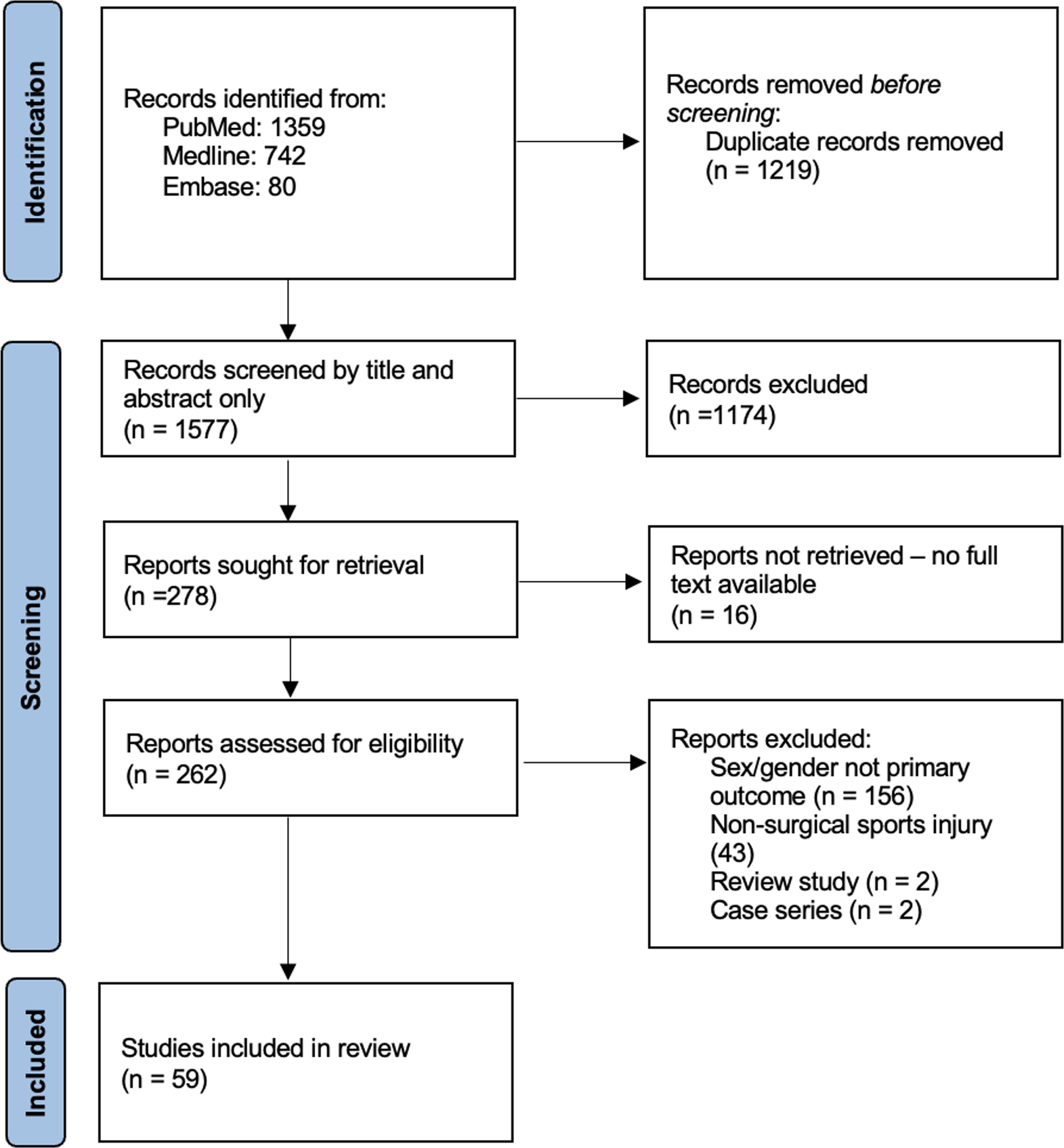
Fig. 3
Final full-length anteroposterior and lateral radiographs of the patient from Figs. 1 and 3 months post-operatively
Deformity analysis during pre-operative planning for knee osteotomies is a multi-faceted process that requires consideration of various anatomical and biomechanical factors to optimize outcomes. Traditionally, the mechanical medial proximal tibial angle (mMPTA) has been a primary tool for pre-operative planning, as it focuses correction around the tibia without being influenced by patient positioning artifacts that may affect measurements like the mechanical femorotibial angle (mFTA) or weight-bearing axis [25, 27]. The mMPTA has also been shown in research to accurately correct limb alignment compared to other measures, such as the weight-bearing line ratio or joint line convergence angle (JLCA) [27]. Along with mMPTA, osteotomy planning should also involve consideration of the mechanical axis deviation (MAD), mechanical lateral distal femoral angle (mLDFA), JLCA, joint obliquity, and sagittal plane measures such as tibial slope and femoral version/tibial torsion. MAD represents the deviation of the mechanical load-bearing axis from the neutral limb alignment and is critical in determining the site of correction. When MAD falls within the metaphyseal regions of the tibia or femur, a single-level osteotomy can be sufficient. However, when MAD is excessively shifted outside the bone boundaries, a double-level osteotomy is often required to distribute the correction while maintaining joint congruency [28]. The location of correction is also influenced by whether the primary issue is pain or instability, with medial compartment osteoarthritis and isolated varus deformity often benefiting from HTO, while valgus malalignment and lateral compartment overload commonly involving DFO. Ligamentous laxity and other instability patterns further determine whether the correction should be performed at the femur, tibia, or both [29, 30], or involve soft tissue repair or reconstruction.
The decision to perform a single or double-level osteotomy is guided by the magnitude and location of the deformity. If a single mMPTA and mLDFA correction must go beyond 95° of mMPTA, this can result in excessive joint line obliquity and increase shear forces on the cartilage, potentially accelerating degenerative changes [31]. Additionally, the JLCA, which reflects coronal plane laxity, can influence whether bony correction alone is sufficient or if additional soft tissue balancing procedures are needed [32].
The choice between opening-wedge and closing-wedge osteotomies depends on the desired correction geometry, the patient’s bone quality, and soft tissue constraints. Open-wedge techniques may require grafting, while closing-wedge osteotomies may have a lower risk of delayed union. PSI has been shown to enhance both techniques by pre-determining wedge dimensions and optimizing hinge placement, which gives surgeons the ability to change both coronal and sagittal alignment with one cut which is easier to perform.
After virtual corrections have been planned, patient-specific cutting guides are designed and created. These are all custom tools tailored to fit the patient’s anatomy intra-operatively. Using the guides intra-operatively is as important as the virtual pre-operative planning, as research has shown that when virtual pre-operative plans are only used as a reference without printed guides, over 20% of patients have post-operative alignment > 3° outside the planned correction [33].
Optimizing the efficiency of image acquisition, processing, and PSI manufacturing is dependent on each surgeon’s practice environment. While some institutions can facilitate this process in-house with 3D core facilities, other surgeons may choose to use commercial companies to help facilitate the process, though this may increase overall costs [24].
Patient models are typically printed using medical-grade resin, polycarbonate, acrylonitrile butadiene styrene, polyethylene terephthalate glycol, and nylon-based materials [34]. The raw materials for PSI can be quite inexpensive, as some authors have reported printing PSI for less than €2.5-5 euro per patient, while an appropriate 3D printer may only cost €500–2000 euros. However, more expensive manufacturers can deliver higher quality guides and models [35, 36]. Ultimately, all PSI must be capable of withstanding the sterilization processes, such as steam pressure autoclaves, gamma rays, or low-temperature hydrogen peroxide sterilization [24].
PSI Surgical TechniqueIntra-operatively, patients are typically positioned supine on a radiolucent table to facilitate fluoroscopic imaging, with a lateral post used to stabilize the limb and a footrest to support the operative leg. In cases requiring lower flexion angles, a trauma bump may be placed beneath the knee to optimize exposure and positioning. Fluoroscopy setup is critical for accurate imaging. For medial osteotomies, the C-arm is positioned on the operative side, while for lateral osteotomies, it is positioned on the nonoperative side to provide optimal visualization and minimize parallax errors. A tourniquet is typically used at the discretion of the surgeon, and tranexamic acid may be administered for assistance with hemostasis.
A standard approach for medial tibial osteotomy involves an inverted L-shaped incision is made on the medial tibia to access the osteotomy site. The pes anserinus tendons are mobilized and protected during the osteotomy, while the MCL is protected by retracting it posteriorly and ensuring it is not detached during the osteotomy. A neurovascular retractor is placed posterior to the tibia after palpating the fibula head from medial to lateral, which helps protect the popliteal neurovascular bundle and other posterior structures from injury during the osteotomy.
In cases requiring femoral osteotomy, medial or lateral approaches can be utilized based on pre-operative planning for opening or closing wedges for either varus or valgus deformity. Standard approaches to the medial and lateral distal femur are used to perform these osteotomies, and care is taken to protect the neurovascular structures. Because patient-specific guides are customized to the patient’s unique bony anatomy, thorough exposure and subperiosteal dissection must be performed to ensure the guides can be placed accurately on the bony surface without soft tissue interposition. In some cases, abnormalities like osteophytes must be removed to ensure guide fit.
After the guide is positioned appropriately, the guides can be held with temporary fixation such as screws or wires. These often have pre-determined lengths that help prevent violating the far cortex. Fluoroscopy can then be used to confirm correct positioning of the guide and compare its intraoperative position with the pre-operative template. Once proper cutting guide placement is confirmed, osteotomy cuts are performed using different techniques depending on the system being utilized. Some systems use drill bit technology for opening HTO, allowing precise control over the cut depth and reducing the risk of hinge fractures [37]. Other systems utilize an oscillating saw blade through the guide, with a predetermined blade depth calculated during pre-operative planning to ensure accurate resection while preserving the integrity of the far cortex. Following the cut or cuts, fluoroscopy is used to verify correct positioning and confirm a far cortex bony hinge. At this point, the wedge of bone can be removed for closing wedge osteotomies, or the gap can be opened and checked with the help of other printed wedge guides in opening wedge osteotomies. Once this osteotomy is completed, an intra-operative mechanical alignment check can be performed, if desired, using a radiopaque marker such as an electrocautery cord or metallic rod. However, this alignment check is generally less necessary with PSI compared to the freehand technique given the inherent accuracy and customized guides used.
Drill holes for the plate can then be made through a guide, and the appropriate length of each screw, which was calculated preoperatively using the CT scan and software, can be confirmed. For opening wedge osteotomies, bone grafting is typically required when the correction exceeds 10°, as it provides additional stability and promote bone healing. For smaller corrections, the use of bone grafts is at the surgeon’s discretion, though it is commonly implemented to enhance stability. Plates used for closing wedge osteotomies can be lower profile and smaller, as the bone surfaces are brought together, reducing the need for more robust hardware. Finally, the plate is secured, and the wound is closed in a standard fashion, ensuring proper soft tissue management and hemostasis.
In some cases, patients may require concomitant procedures alongside osteotomy, such as osteochondral allograft transplantation, meniscus root repair or transplantation and/or ligament reconstruction, and thus, the osteotomy must be performed with these additional procedures and sequences in mind [38,39,40,41]. One major advantage of PSI in this context is its ability to facilitate precise preoperative planning for complex procedures to avoid tunnel convergence, such as when drilling multiple tunnels for a meniscus root repair with and concomitant ACL reconstruction [42].
Some tips for success using PSI include:
Bring pre-operative 3D models or printed templates to the OR for reference throughout surgery.
Ensure guides have appropriate labels including side (left or right), degree of correction, and patient identifiers.
Expose bony landmarks adequately and protect neurovascular structures.
Verify the location of the guide with both anatomical landmarks and with fluoroscopic imaging to ensure proper placement prior to making cuts.
Advantages and Limitations of PSIPSI guides are unique to a patient’s bony anatomy, and pre-operative planning allows surgeons to determine the location and depth of cuts, size of wedge, and screw sizes prior to surgery, which research has demonstrated increases precision, decrease OR time, and fluoroscopy exposure.
Accuracy of CorrectionPSI guides ideally improve the accuracy of planned osteotomies by setting a defined starting point and angle for the bone cuts and defining the planned gap size. Victor et al. published one of the earliest studies on the use of PSI for HTO and DFO and found that in a 14-case series the accuracy of post-operative correction was 0° ± 0.72 mFTA and all cases were within +/- 1° of the planned coronal plane correction, while a study by Munier et al. found < 2° of difference between planned and achieved correction in 19 out of 20 coronal or sagittal corrections [16, 25]. A large case series published by Chaouche et al., including 100 opening-wedge HTO cases, found an accuracy of 1.0° ± 0.9 for mFTA, 0.5° ± 0.6 for mMPTA, and 0.4° ± 0.8 for tibial slope [43]. Another series by Zaffagnini et al. found in 25 patients undergoing HTO with PSI, the mean difference between planned and achieved HKA and PTS was 2.1° ± 2.0° and 0.2° ± 0.4°, respectively [44]. Studies examining more complex procedures, including double-level osteotomies around the knee, have also reported successful and accurate use of PSI [45].
Studies comparing PSI to traditional freehand techniques have also found a superiority in correction accuracy with PSI use. Pérez-Mañanes et al. found that between 20 control patients using traditional techniques for opening wedge HTO compared with 8 cases using PSI, the mean difference between planned and post-operative wedge angle was 1.1° (0°–2.8°) using the conventional technique and 0.5° (0°–1.2°) using PSI [35]. Similarly, Arnal-Burró found in 12 DFOs that the mechanical axis deviation in the coronal plane was, on average, 0.28° mFTA (ranging 0°–1°) with PSI and 1.8° mFTA (ranging 0°–4°) without PSI [36]. Kim et al. found in 20 cases of HTO that the mean absolute difference between planned and achieved correction in the PSI group was 2.3% ± 2.5 to the target point in the weight-bearing line, compared to the conventional technique group of 6.2% ± 5.1 [46]. In a retrospective study of 49 patients undergoing medial opening-wedge high tibial osteotomy with PSI versus 38 with the conventional technique, Fayard et al. found that accuracy of ± 2° in the HKA was achieved in 44 (90%) in the PSCG group and 24 (65%) in the standard group [47]. Recently, a systematic review of 14 studies of PSI for medial opening wedge HTO found the operative accuracy to be within 0.6° of the pre-operative plan on coronal and sagittal planes, as well as an average error within 0.8° of the planned hip-knee correction angle [48].
In addition to precision, Aman et al. reported that rates of correction outliers ranged from 0 to 25% across eight studies utilizing 3D-printed PSI [49]. Although few studies have reported outlier rates on conventional opening wedge HTO, several have reported rates above 30%, with outliers correlating with poor patient-reported outcomes and the deterioration of knee function [50,51,52]. A 2020 meta-analysis found insufficient evidence to determine if PSI could reduce post-operative outliers compared to traditional techniques, but the rate in the PSI group was reported to be 15% [50].
Despite many articles in the literature supporting greater precision of correction with PSI, several studies have challenged this idea. A study by Abdelhameed et al. found in a retrospective review of patients undergoing knee osteotomies of 50 patients with freehand and 41 patients with PSI technique that there were no statistically significant differences between the target correction and the obtained correction in both groups for any radiologic measurement of alignment [53]. The authors concluded that in experienced hands PSI may not offer any significant benefit. In a study by Tardy et al., 126 patients were prospectively divided into conventional, navigation, and PSI groups. The authors found that in terms of precision, PSI was only significantly improved compared to navigation and not the conventional technique [54].
Operative Time and Fluoroscopy ExposureSeveral studies have included intra-operative variables that may improve with PSI, including operative time and number of fluoroscopy shots taken. Studies have typically found that PSI decreases both OR time and fluoroscopy used intra-operatively. Mao et al. observed an overall reduction in OR time with PSI of 16.8 min during medial opening wedge HTO, while Pérez-Mañanes et al. reported a reduction of 31 min, and Stimolo et al. found a difference of 10.17 min [35, 55, 56]. Similarly, Arnal-Burró et al. found that PSI reduced OR time by 32 min [36].
Regarding fluoroscopy exposure, Mao et al. found an average of 2.8 fewer fluoroscopy exposures using PHI compared to conventional techniques [55]. Stimolo et al. found an overall reduction of 7.41 shots for PSI [56], while Pérez-Mañanes et al. found that the average fluoroscopic image count was 55 for conventional and 8 for PSI, a reduction of 47 [35].
CostA current limitation of PSI is its associated cost. 3D printing is associated with a considerable upfront cost. However, because 3D guides have been observed to decrease operating time, and costs associated with complications may be avoided at a higher rate, the cost 3D printing may be justifiable [57]. Arnal-Burró estimated in their study that cost savings from decreased OR time using PSI was equivalent to €415/procedure, even after considering the added costs of pre-operative CT scan and materials for PSI [36]. Depending on the infrastructure or companies used during preparation, associated pre-operative imaging, design, and processing costs are likely highly variable across institutions.
Patient Reported OutcomesWhile many studies have looked at the provision of correction and intra-operative variables with PSI for knee osteotomies, some have also investigated whether these benefits may translate into superiority in patient-reported outcomes. Research has shown that patient-reported outcomes are improved after knee osteotomies using conventional techniques and PSI [43, 58]. Using PSI, Chaouche et al. observed significant improvements in Knee Injury and Osteoarthritis Outcome Score (KOOS) Pain, KOOS symptoms, KOOS ADL, KOOS, sports/rec, KOOS QOL, and UCLA activity scale scores compared to pre-operative scores [43].
Several studies also report direct comparison between PSI and traditional techniques. In a comparative study between PSI and freehand technique for HTO, Gao et al. found that clinical and functional American Knee Society clinical scores were significantly better in the PSI group at 3 and 6 months postoperatively but that both groups had equivalent scores at final follow-up [59]. Similarly, in a prospective study of 18 patients who underwent medial open wedge high tibial osteotomy using PSI versus 19 who underwent a traditional technique, the authors found significantly higher subjective IKDC scores and Lysholm scores in the 3D-printed group at the 3-month follow-up but not significantly different at other time points [55]. Abdelhameed et al. found in a retrospective review of patients undergoing knee osteotomies of 50 patients with freehand and 41 patients with PSI technique that there were no statistically significant differences in any of the 2-year follow-up KOOS sub-scores [53]. While studies support the clinical efficacy of using PSI for knee osteotomies, there may not be any long-term clinical benefit in patient outcomes, however more research is needed in this area.
ComplicationsOverall, complications after knee osteotomies using PSI are low and range between 0 and 13% [9, 16, 25, 43, 47, 55, 59,60,61,62]. Complications using PSI are similar to those after knee osteotomies using traditional techniques and include tibial slope changes, hinge fractures, infections, delayed union, and non-union [47]. Thus far, comparative studies also report no significant difference in the complication rate between PSCG and standard techniques [16, 25,
Comments (0)