
Remember me


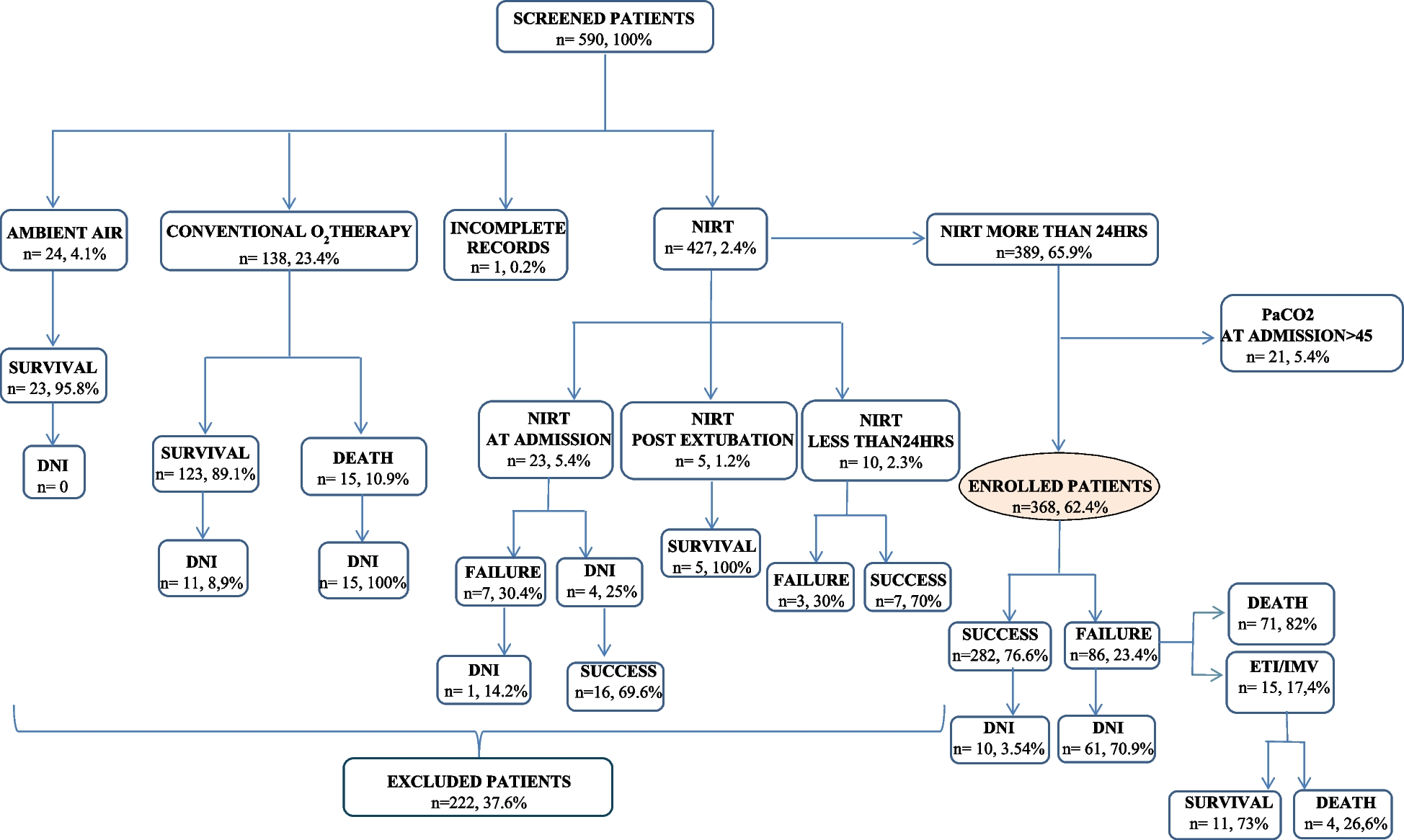

During the inclusion period, 162 patients with community-acquired LP were enrolled from 12 French ICUs. 87 patients (54%) were directly admitted to an ICU while 75 (46%) had previously been admitted to another department with a median stay of 2 days [1,2,3].
The median age was 61 years, and 120 patients (74.9%) were male. 79 patients (48.8%) were smokers, 52 (32.1%) were alcohol drinkers. 32 (19.8%) had cardiomyopathy, 21 (15.9%) had diabetes, 18 (11/1%) had neoplasia and 16 (9.9%) had Chronic Obstructive Pulmonary Disease (COPD) while only 28 patients (17.3%) had immunodepression or hemopathy. The median time between symptom onset and hospital admission was 5 days [3,4,5,6,7].
Infection characteristics (Table 1)Fever at admission affected 143 patients (88.8%) while 135 patients (83.3%) had suffered from acute respiratory failure, and 54 patients (33.3%) had mental confusion. 37 patients (22.8%) were in septic shock on admission. Median SOFA was 5 [3,4,5,6,7,8].
Hyponatremia was present for 95 patients (59%) and hepatic cytolysis for 96 patients (60.4%).
A large number of types of radiological focus were observed (Table 2).
Table 2 Radiological focus (n = 162)Diagnosis of LegionellaLegionella diagnosis was made by Urinary Antigen Test for 144 patients (88.9%). 2 patients were diagnosed by Legionella serology, including one post-mortem (Table 3). The diagnostic samples were obtained by bronchoalveolar lavage (BAL), broncho-aspiration or sputum, and analyzed by culture in 8 patients (4.9%) and by BAL or nasal polymerase chain reaction (PCR) in 7 patients (4.9%). Median time between hospitalization and diagnosis was 1 day [0–2].
Table 3 Diagnosis method (n = 162)Antibiotic treatmentMedian time from hospital admission to administration of antibiotic against Legionella introduction was 0 days [0–1]; 156 patients (96.3%) received at least one antibiotic against Legionella on t admission to an ICU.
One hundred twenty-eight patients (79%) were treated with combination therapy. The most commonly used combination therapy was fluoroquinolone and macrolide (118 patients), (Table S1). Median combination therapy duration was 10 days [7,8,9,10,11,12,13,14,15], followed by mono-therapy for 67 patients. 33 patients (20.4%) received monotherapy only, 22 a fluoroquinolone and 11 a macrolide. Median antibiotic duration was 18 days [14,15,16,17,18,19,20,21]. One patient died on the day of ICU admission, before antibiotic treatment could be administered.
Time course of disease (Table 4)Table 4 Outcomes, length of stay and therapeutics (n = 162)Invasive ventilation was used for 95 patients (58.6%), of whom 79 were intubated during the first 24 h after ICU admission. 16 patients were intubated later in their hospital course, with a median of 2.5 [2-3.5] days between ICU admission and intubation. 73 patients (76.8%) had acute respiratory distress syndrome according to the Berlin definition [21]. Median invasive ventilation duration was 10 days [6,7,8,9,10,11,12,13,14,15,16,17]. Among ARDS patients, 65 received neuromuscular blocking agents and 39 were placed in a prone position.
Only 9 patients (5.6%) received non-invasive ventilation (NIV), 21 (13%) required high-flow nasal oxygen therapy (HFOT) only and 4 (2.5%) required a combination of NIV and HFOT. Veno-venous extracorporeal membrane oxygenation was performed in 8 patients.
Median ICU stay duration was 11 days [5,6,7,8,9,10,11,12,13,14,15,16,17,18,19], and the median hospital stay duration after ICU admission was 17 days [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29].
Survival analysisAt 28 days, 19 patients (11.7%) had not survived, and were analyzed in the univariate and multivariate analysis. 2 other patients died after 28 days and before ICU discharge. Univariate analyses are available in the Supplementary Appendix (Table S2).
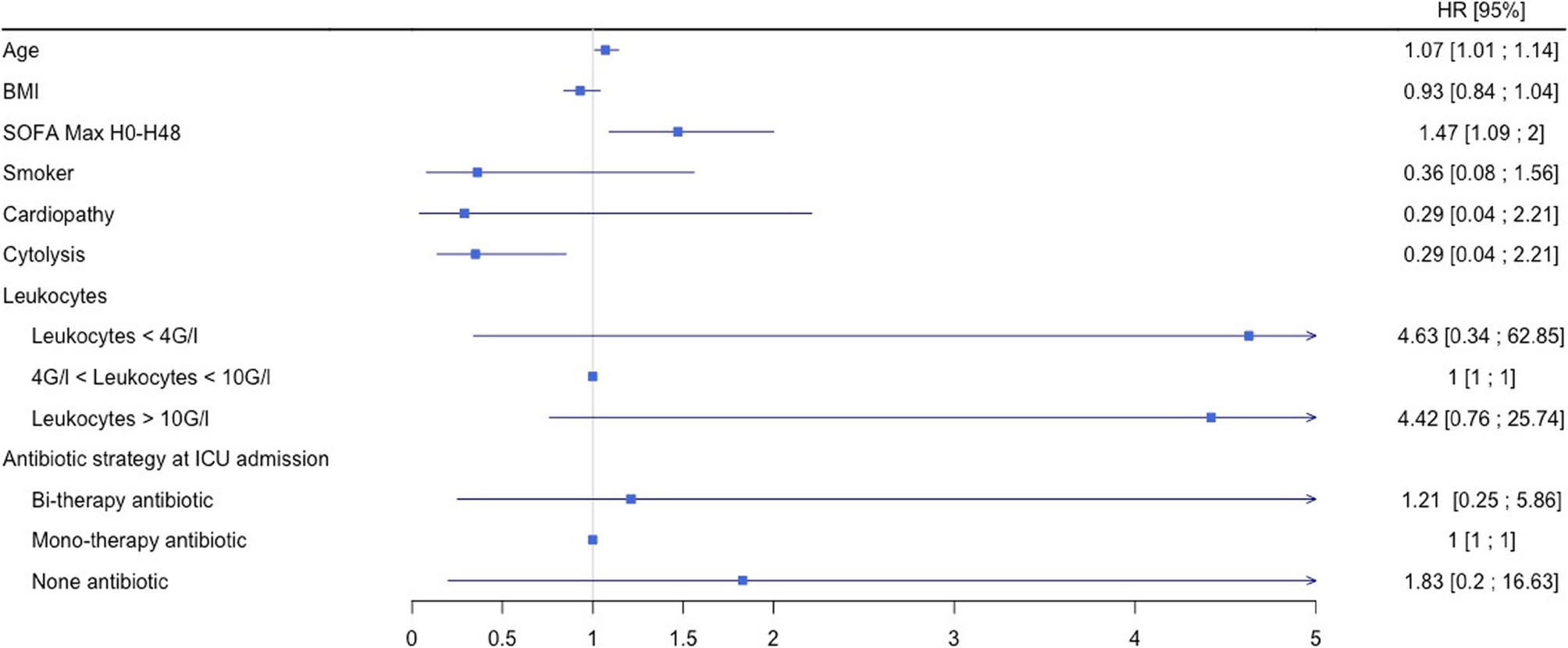
In multivariable analysis (Table S3 Fig. 1), age (HR, 1.07; 95% CI, 1.01–1.14) and a high SOFA (Sequential Organ Failure Assessment) score during the first 48 h (HR, 1.47; 95% CI, 1.09-2) were significantly associated with mortality (Table S3 and Fig. 1). No comorbidities were found to be correlated with increased mortality. Among biologic parameters, cytolysis was a protective factor (HR, 0.35; 95% CI, 0.14–0.85). Lack of antibiotics at ICUs admission was not associated with mortality.
Fig. 1
Risk factors for mortality at D-28 after admission to ICU for LP (n = 19)
Length of stay in an ICULength of stay was analyzed for 141 patients who were discharged alive from an ICU. Univariate analyses are available in the Supplementary Appendix (Table S4).
In multivariable analysis (Table S5, Fig. 2), only the number of comorbidities (Incidence Risk ratio: IRR, 1.17: 95% CI, 1.05–1.29), high SOFA score during the first 48 h (IRR, 1.14; 95% CI, 1.10–1.17) and no antibiotics on ICU admission (IRR, 2.04; 95% CI, 1.14–3.62) were significantly associated with ICU length of stay.
Fig. 2
Multivariate analysis of length of stay in ICU (n = 141)
Ventilator-free days at 60 daysVentilator-free days were analyzed for 95 patients having received invasive ventilation. Univariate analyses are available in the Supplementary Appendix (Table S6).
In multivariate analysis (Table S7, Fig. 3), only the high SOFA score during the first 48 h was significantly associated with ventilator-free days (IRR, 0.95; 95% CI, 0.91–0.99).
Fig. 3
Multivariate analysis of ventilator-free days at 60 days (n = 93)
Comments (0)