In this study, we combined 4DCT image data and a DSM framework to compute the strains of the RVOT/PA during the cardiac cycle in a population of 20 patients undergoing TPVR. The DSM allowed quantification of the average distributions of circumferential strains, axial strains, and strain ratio across the population along the RVOT/PA. Overall circumferential strains, due to the diameter increase during systole, are considerably smaller (half) than axial strains required to accommodate the stroke volume. While strain ratios were predominantly positive – indicating that the RVOT/PA simultaneously dilates and elongates in systole – some regional differences were noted: the proximal RVOT presented the largest elongation (positive axial strains) together with some compression (slightly negative circumferential strains). The elongation in systole decreased along the pulmonary valve and pulmonary trunk, while these regions simultaneously dilated, with the distal region being the most dilated in systole. This led to an increased strain ratio along the RVOT, slightly larger than 1 in the pulmonary trunk. The proposed analysis can improve our understanding of the RVOT/PA loading conditions to support new TPVR device designs, as manufacturers could provide solutions that account for these complex dynamics.
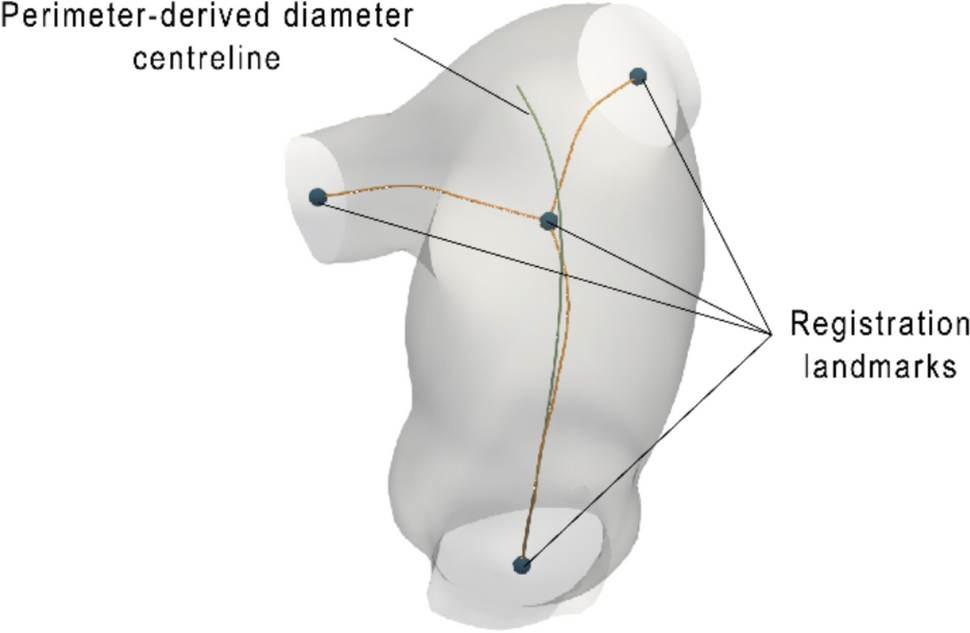
The patients for the presented study were selected based on their need for a new pulmonary valve, with the cohort including predominantly patched and native RVOTs after valvotomy/valvuloplasty repairs. These patients present with a wide range of anatomies [2], highly dilated, often resulting in severe regurgitation, and also exhibit large dynamics [2, 9]. Indeed, the cohort overall RVOT/PA volume increased by 49% during systole (surface area by 29%) due to a simultaneous increase of 11% in RVOT/PA diameter and 26% in length. This average magnitude of length change in the population is similar to what has been previously found in the normal population [10] but with a much larger spread. However, measures of volumes, diameters, and lengths, do not provide local or regional RVOT/PA surface strain information and differences among patients. Additionally, routine clinical measurements of the RVOT/PA from CT scans [10, 24], especially in terms of diameters, are prone to errors as sensitive to operators’ choices on the cross-sectional planes. Thus, the proposed DSM, with no need for operator dependent measures and anatomical landmark selection, difficult in the context of repaired CHD, was developed to capture automatically the RVOT/PA complex surface deformations that happen in this group of patients.
Our group has previously shown the importance of 4D imaging for examining RVOT/PA geometry changes during the cardiac cycle to assess device implantation parameters [9]. 4DCT has become the standard imaging modality for patient screening for the next generation of TPVR devices, particularly through derived perimeter plots. These and similar methods used to quantify strain in the great arteries [10, 25], provide limited information, discarding most of the 4D details contained in the images. DSMs, instead, may provide an alternative measure to capture the entire 4D information for more comprehensive clinical screening. For example, in this study, we highlight the regional variations of circumferential strains, largest in the distal and anterior regions of the RVOT/PA. These regions of high circumferential strain, particularly in the distal region, may indicate areas at risk of poor device apposition or device migration. This is particularly important in cases where the TPVR device is deployed more distally than normal. On the other hand, regional differences in the axial strains, largest in the proximal and anterior regions of the RVOT/PA, are considerable and present additional load on the TPVR stent in this region. Furthermore, the median axial strain maps show reduced axial and circumferential contraction in the proximal, anterior region which may indicate the overall effect of passively deformed patch tissue.
Furthermore, the DSM methodology presented here is applicable to other 4D imaging methods such as modern 4D cine magnetic resonance imaging. This is important as centers seek avenues that reduce exposure of patients to ionizing radiation. With further investigations on larger cohorts, development of DSM methods that can be implemented in the clinical workflow, and the growing market of new available TPVR devices, these models may be able to support better patient screening and device selection for optimal outcomes.
4DCT in these patients was performed for the purpose of screening for newer self-expanding valve platforms (Harmony, Medtronic, Minneapolis MN; Alterra, Edwards Life Sciences, Irvine, CA; Venus P-Valve; Venus Medtech, Hang Zhou, China). These are designed for native RVOT/PAs and are based on diamond-like cell shapes and circular cross-sections of varying diameters along the length [4]. These designs force the devices to shorten during dilation, in disagreement with the natural dynamics of the unconstrained RVOT/PA identified in this study. Hence, TPVR results in stiffening of the RVOT/PA not only in the radial direction, as already widely reported, but, mostly in the axial direction. By altering the afterload compliance, this may, on one hand, affect the ability of the RVOT/PA to accommodate the cardiac stroke volume, thus impacting on the overall hemodynamics performance. On the other hand, axial stiffening of the RVOT/PA may transfer the cyclic axial loads to the TPVR stent, thus increasing the risk of fatigue failure and reducing the lifespan of the device [26]. More natural RVOT/PA deformations could be achieved considering new auxetic TPVR device designs [27, 28] that allow for more flexible solutions with greater axial elongation when dilating and asymmetric designs that can accommodate strain ratio regional differences, as indicated in this study.
Furthermore, not only the designs of the TPVR devices, but also the standards for assessment of their mechanical and long-term performance should consider more realistic loading conditions. Stent mechanical performance testing focuses, among others, on radial stiffness and ability of the device to withstand cyclic fatigue based on hydrodynamic pulsatile loading conditions that replicate physiologically relevant diameter changes. However, no tests are purposely carried out to assess the mechanical behavior when the device is loaded in the axial direction. Current standard tests, that may be suitable for other stent applications or transcatheter aortic valve implantation (TAVI) devices – the aortic root in TAVI patients is often stiff and calcified – do not account for the complex range of in vivo loading conditions encountered in TPVR patients.
As the database of 4D scans increases with more patients screened for TPVR, there is a growing opportunity to expand image post-processing methods such as DSMs to study in situ RVOT/PA dynamics. This would benefit future TPVR device designs and may provide further clinical insight for TPVR patient selection criteria.
Limitations
This study includes a small sample of patients with different diagnosis and RVOT/PA repair types. The size of the cohort and number of patients in each sub-group of repair type do not carry sufficient power to characterize completely the population or its sub-groups. The results hence present evidence to support commonly observed dynamics and motivate a larger study to find differences between sub-groups of RVOT/PA repairs.
Segmentation model processing for DSM construction included steps for smoothing and mesh refinement of the segmented surfaces. Errors due to these operations and created by the DSM itself were smaller than the CT images’ voxel size, and, therefore, considered acceptable.
Our proposed methodology computed the strains between two time points over the cardiac cycle (end of systole and end diastole). These strains do not necessarily provide insight into the maximum axial or circumferential strains over the cardiac cycle, due to regional and individual variations [9]. Extending the image analysis to include multiple phases may uncover higher strains in RVOT/PA loading, more relevant for TPVR.
Additionally, the computed strains are not absolute, but rather relative to the end-diastolic phase, which was chosen as reference, as the developed model does not take into account the pre-strains experienced by the RVOT/PAs at diastole. Computing the pre-strain state requires complex inverse modeling approaches with several material/loading condition assumptions, and was outside the scope of this study. Hence the computed strains should be considered as relative and not a representation of the total biomechanical state of the RVOT/PA, limiting considerations on the overall tissue biomechanical response.
Strains in the RVOT region show predominant axial elongation which has been previously described [29]. Furthermore, analyzing population and region averaged strain measurements limits the ability to asses the impact of the presence of a patch, adhesions or sutures on local, patient-specific, strains. The results presented here are intended to be population level characteristics and focus on the fact that prominent axial strains exist in the population.






Comments (0)