Study type and population
The study was divided into three distinct parts:
1.
An observational audit of professional practices assessing the compliance of operator attire in the operating room during breast surgeries, conducted from May 30 to July 5, 2024, at the South Hospital Group (GH Sud) of the Hospices Civils de Lyon (HCL), Pierre-Bénite, France.
2.
An observational audit assessing the compliance of patient preoperative skin preparation for all breast surgeries during the same period, from May 30 to July 5, 2024, at the GH Sud, Pierre-Bénite, France.
3.
A retrospective case-control study nested within a prospective cohort of patients who underwent breast surgery at the GH Sud of the HCL, Pierre-Bénite, France, between January 1, 2019, and June 1, 2024.
In 2024, our facility had 1062 hospital beds, accommodating 43,788 admissions for full hospitalization and outpatient care. The GH Sud has three gyneco-obstetric operating rooms and a gyneco-oncology surgical hospitalization unit with 22 full hospital beds equivalent to 2161 patient’s admissions.
Eligibility criteria
For all three parts of the study, we included all adult women undergoing breast surgical procedures at GH Sud of the Hospices Civils de Lyon in Pierre Bénite, France. These procedures encompassed total or partial tumorectomy, total or partial mastectomy (with or without lymph node dissection), regardless of hospitalization type (conventional or ambulatory) and with or without antibiotic prophylaxis, as specified by the national protocol for the prevention of surgical site infections [20].
For the audit on operating room attire, were included all professionals present in the operating room from the time the patient entered the operating room until the incision.
For the case-control study, cases were defined as patients who developed a SSI within 30 days following surgery. A SSI was defined by any positive microbiological sample, superficial or deep, taken for diagnostic purposes at the surgical site, with one or more isolated microorganism(s), and performed within 30 days following the target surgical procedure during the index surgical stay or upon readmission, further validated by a surgeon. The surgical site is defined as the site of the surgical incision or any anatomical site in contact with and/or manipulated during the target surgical procedure according to the French protocol for the surveillance of SSIs [21]. Cases without samples taken or with sterile cultures were excluded from this study. Controls were patients who did not develop an SSI within 30 days of the surgery. SSIs were detected by the system implemented by the GH Sud infection control unit, which involved cross-referencing data from the Medical Information Systems Program of patients who underwent surgery with microbiology laboratory data filtered for clinical samples such as wound swabs, suppuration, abscess, lymphocele, or wounds during post-operative follow-up consultations. The results were then compared and analyzed to identify risk factors associated with SSIs.
Data collection
For the audit on operating room attire, information regarding attire, cap wearing and type, surgical mask use, and hand hygiene requirements (notably the absence of jewellery) was collected using the standardized evaluation grid adapted from the national recommendation for the operating room attire [13]. Healthcare workers could be observed more than once.
For the skin preparation audit, information was collected using the standardized evaluation grid from the 2024 Pre-OP audit of the national surveillance mission on surgical and interventional procedures (SPICMI) [22]. Care practices were classified into four themes, in accordance with the latest recommendations: preoperative shower, hair removal, skin cleaning, and antisepsis/skin disinfection.
For the case-control study, data on age, gender, Body Mass Index (BMI), operating room, surgery duration, type of procedure, antibiotic prophylaxis, American Society of Anaesthesiologists (ASA) score [23], Altemeier classification [24], and National Nosocomial Infections Surveillance System (NNISS) score [19] were prospectively collected for both cases and controls following the national methodology [20, 25]. Comorbidities such as diabetes, hypertension, immunosuppression, respiratory diseases, malignancies, and renal or liver conditions were recorded. Lifestyle data included active smoking at the time of surgery, chronic alcoholism, and drug addiction.
Preoperative and clinical data included length of preoperative hospital stay, the oncological nature of the surgery, isolated fever, preoperative infection, emergency surgery context (not scheduled 24 h before surgery), and the placement of a harpoon for marking the excision zone.
Data on the traceability of SSI prevention measures included antiseptics used for patient skin preparation and antibiotic prophylaxis. Surgery-related data included the order of the procedure on the surgery schedule. Postoperative data included removal of dressing, surgery duration, total length of hospital stay and in-hospital death.
Data specific to SSIs included the date of the sample, the bacterial species and its resistance profile, the type of SSI (superficial, deep or organ/space infection), the delay to SSI onset, and reoperation for SSI.
Data were collected by two surveyors specifically trained for the purpose of this study. Data from the audits on operating room attire compliance and patient skin preparation were obtained via direct visual observation of professionals and practices, respectively. Some fields (preoperative shower) required direct questioning of the patient or, if not possible, the State-Certified Operating Room Nurse, or, as a last resort, consulting the traceability in the patient’s medical record to complete the questionnaire.
For the case-control study, data were collected from the electronic medical records. Data were entered via a secure RedCAP® electronic form (https://redcap.chu-lyon.fr/redcap/).
Statistical data analysis
For the case-control study, each case was randomly matched with two controls over the years (2019, 2020, 2021, 2022, 2023, and from January 1 to June 1, 2024) and by age (age groups of 10 years). The required number of subjects was calculated for a risk difference of 3 between the two groups, with a 20% exposed control population, with obesity as the exposure of interest [11]. Descriptive analyses were performed for the three parts of the study. For quantitative variables, medians (interquartile ranges) or means (standard deviation) were reported depending on normal distribution. Qualitative variables were expressed as numbers (n) and percentages (%). For the case-control study, in univariate analysis, contributing factors were compared between cases and controls using non-parametric Wilcoxon tests, and Pearson’s Chi-squared test or Fisher’s exact test if the Chi-squared test assumptions were not met. Variables with a p-value below the 0.1 threshold in univariate analysis were included in a multivariate model. Multivariate analysis was performed using logistic regression [26].
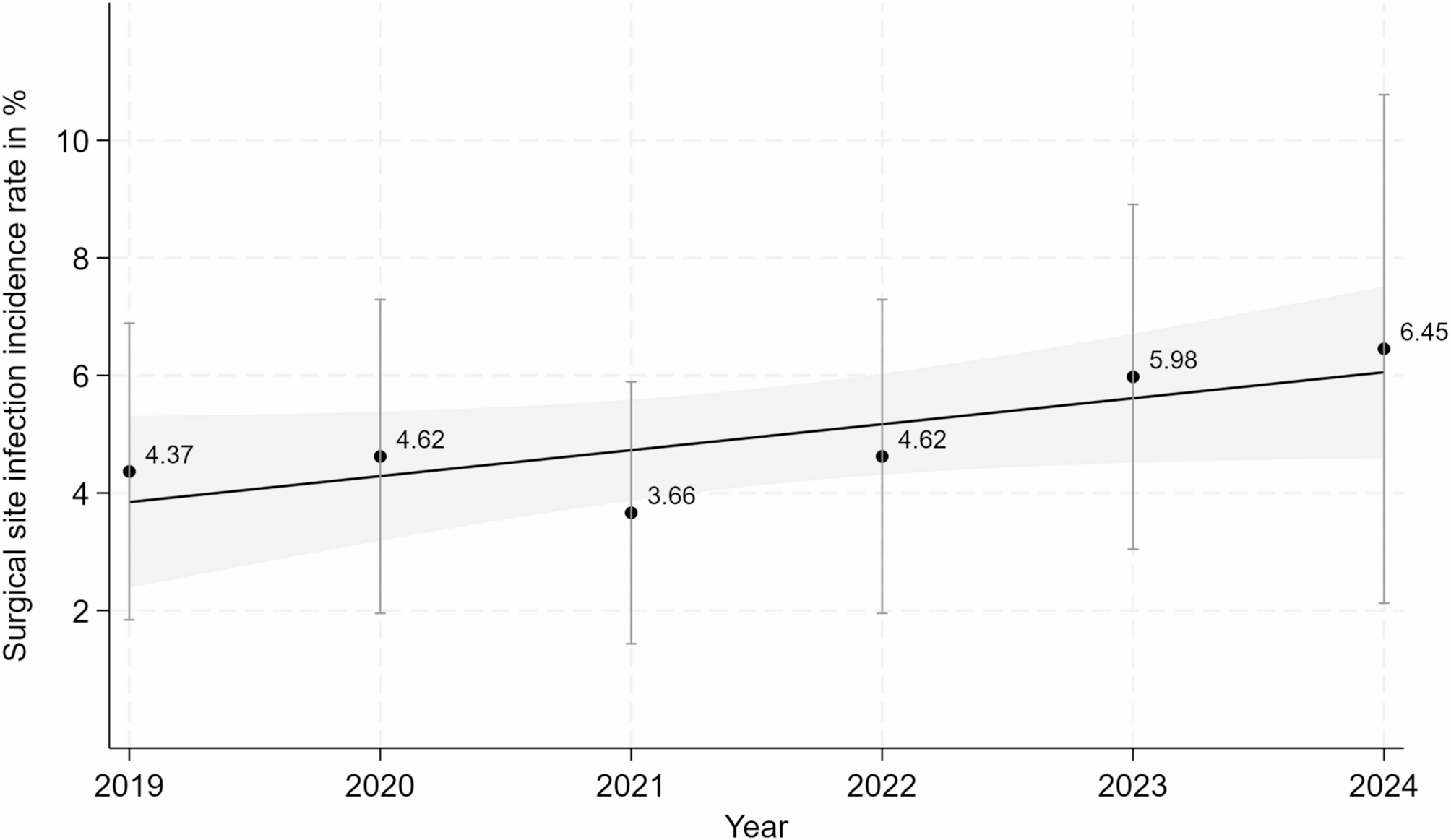
Comparative analysis results were expressed as Odds Ratios (OR) with 95% confidence intervals (CI). The statistical significance threshold was set at 0.05. SSI rates were expressed as cumulative incidence rates per year (number of SSIs per 100 surgeries, %) with 95% CI. The trend in SSI incidence rates over time was analyzed by testing the slope of the linear regression. These statistical analyses were performed using Stata® version 18.0.



Comments (0)