
Remember me


Retrospective analysis was performed on patients originally enrolled into a prospective observational study, CONDUCT–TAVI (ACTRN1261001700820). CONDUCT–TAVI recruited consecutive patients undergoing TAVR at two high-volume centres in Sydney, Australia, between October 2021 and December 2023. Patients were excluded if they had a prior permanent pacemaker (PPM) or aortic valve surgery. Furthermore, if a PPM was not required post-procedure, all patients received an implantable loop recorder prior to discharge. Further detailed information on the CONDUCT–TAVI protocol is publicly available [8]. The protocol has been approved by the Northern Sydney Local Health District Ethics Committee.
The CONDUCT–TAVI cohort was chosen for this study due to the availability of extended rhythm monitoring, which was deemed necessary due to the inclusion of patients receiving self-expanding valves.
TAVR procedureAll patients underwent “minimalist” TAVR, which was performed under conscious sedation via the transfemoral route. Secondary access was either transradial or transfemoral, and single transfemoral transvenous access was obtained for a multipolar electrophysiology catheter for immediate pre and post TAVR targeted electrophysiology study, as mandated by the CONDUCT–TAVI research protocol. Rapid ventricular pacing was performed over the left ventricular wire in all cases. Cerebral protection devices were not used.
Pre-dilatation, valve type and size, as well as post-dilatation was at the implanters’ discretion. All patients were discharged to a coronary care unit with continuous cardiac monitoring for a minimum of 24 h. All patients had an immediate post-procedure, 4-h and 24-h ECG, and underwent standard pre and post procedure echocardiography (day 0 and day 1).
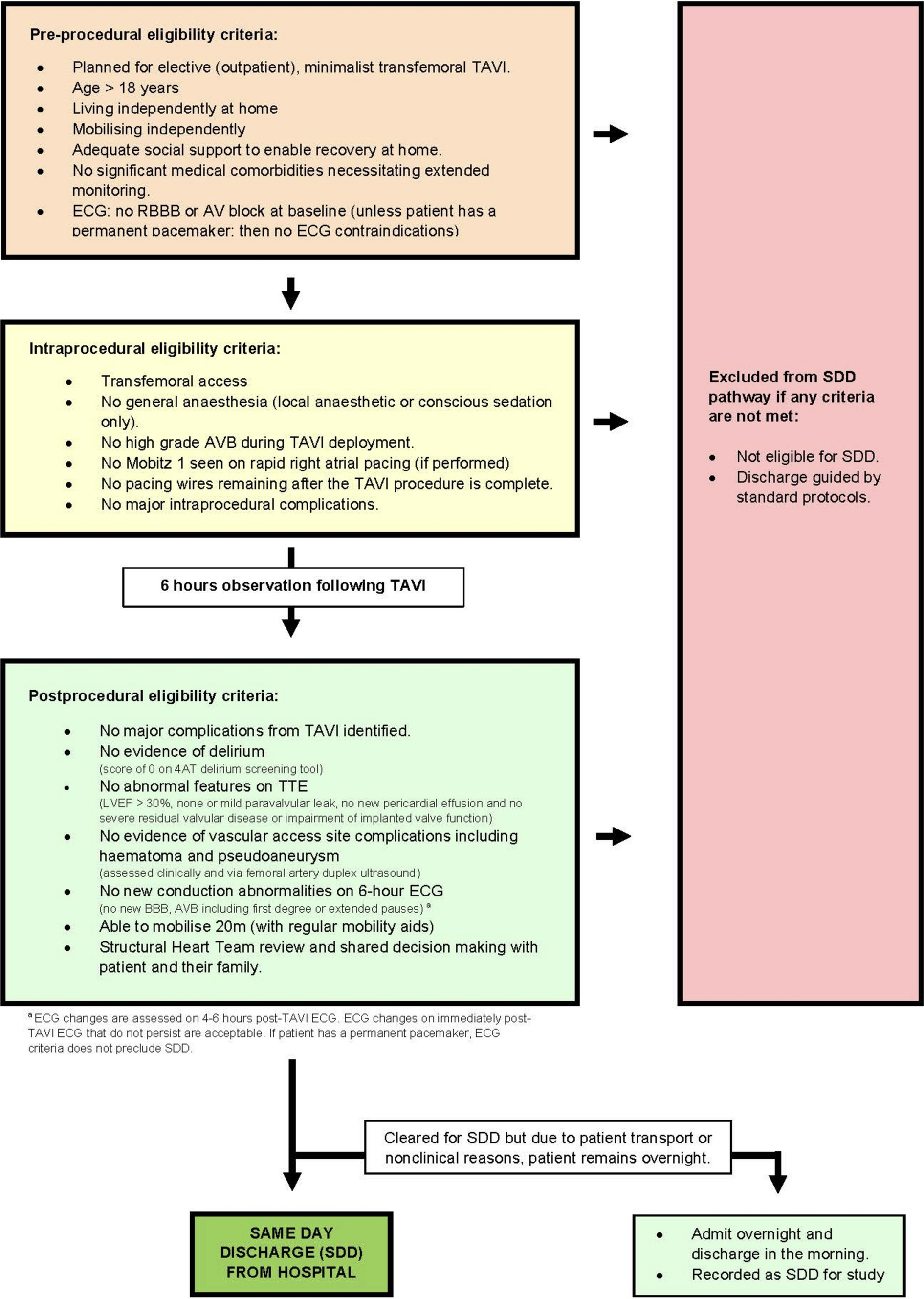
North Shore Day Stay clinical pathwayThe North Shore Day Stay clinical pathway (the ‘North Shore Pathway’) was adapted from previously published protocols [4, 5, 9]. It was retrospectively applied to all patients enrolled in CONDUCT–TAVI to assess theoretical suitability for SDD. The protocol included comprehensive preprocedural, procedural and postprocedural criteria, as illustrated in Fig. 1.
Fig. 1
NORTH SHORE DAY STAY TAVI clinical pathway
Preprocedural inclusion criteria included non-urgent, elective TAVR, age ≥ 18 years, mobilising and living independently, adequate social supports to facilitate recovery at home and no significant medical comorbidities that necessitated additional in-hospital monitoring, such as end-stage renal disease or advanced dementia. Other exclusion criteria were all conduction-related and derived from the baseline ECG. These included a pre-existing right bundle branch block (RBBB) or atrioventricular block (AVB) (first, second or third degree). Whilst the North Shore pathway provides an exception for patients with a prior PPM from conduction-related exclusion criteria, this was not applicable in our cohort.
The procedural requirements were the use of conscious sedation (no general anaesthesia), and the absence of any HGAVB during valve deployment. Furthermore, patients were required to have no recorded intraprocedural complications as per the Valve Academic Research Constorium-3 (VARC-3) criteria [10], and temporary pacing wires were required to be removed prior to the end of the case.
Postprocedural requirements were assessed at 4–6-h post-procedure and included: (1) no evidence of delirium, (2) no evidence of vascular access site complications, such as haematoma or pseudoaneurysm, (3) no abnormal transthoracic echocardiogram features (LVEF > 30%, none or mild paravalvular leak, no new pericardial effusion and functioning implanted valve), (4) no new conduction abnormalities (new AVB, including first degree block, or any new bundle branch block) unless patient had a permanent pacemaker, (5) ability to mobilise 20 m (assessed with the patient’s regular mobility aids) and (6) multidisciplinary team agreement of suitability for SDD.
Given the retrospective nature of this study, evidence of delirium and vascular access site complications were determined by clinical assessment which was established from medical documentation. Other studies investigating SDD in TAVR patients have used clinical examination to assess for delirium and vascular access site complications [4, 5]. Similarly, mobility criteria were also assessed using medical, nursing, or allied health clinical documentation. Patients that were documented to have independently mobilised, for example, to the bathroom outside the room, were considered to have satisfied mobility criteria. Patients that remained on bedrest, required use of a bedpan, or had no explicit mention of their mobility, were considered not to have satisfied mobility criteria.
Assessment for SDD eligibility aimed to replicate real-time decision making by restricting investigators to information only available at each timepoint (pre-TAVR, immediately post-TAVR and 6-h post-TAVR), and blinding to all subsequent in-hospital events and 30-day events.
Patients who met all preprocedural, procedural and postprocedural criteria outlined in the clinical pathway were allocated to the SDD cohort. Patients who did not satisfy one or more criteria were allocated to the standard discharge cohort.
Outcome measuresDetailed patient demographics were obtained and compared between SDD and standard discharge groups. This included age, sex, body mass index and the Society of Thoracic Surgeons–Predicted Risk of Mortality (STS–PROM) score, along with medical comorbidities, prior cardiac procedures, and echocardiographic data. Baseline electrocardiography was also recorded.
Outcomes measured were in-hospital and 30-day post-discharge events, which were defined as per the VARC-3 criteria [10]. The 30-day post-discharge events were defined as occurring following discharge and up to 30 days after their procedure, and included death, hospital re-admission (any cause, cardiovascular and non-cardiovascular), timing of readmission, and detailed post-discharge events, including new permanent pacemaker implantation (PPMI), stroke, vascular access complications, bleeding, delirium and myocardial infarction.
As an additional timepoint, outcomes were recorded in the SDD cohort at the median discharge day of the standard cohort. This aimed to assess whether patients selected for SDD developed complications during the period they would have otherwise remained in hospital, to evaluate the clinical benefit of extended inpatient monitoring in this cohort.
Statistical analysisStatistical analysis was performed using IBM SPSS Version 29.0. Categorical variables were assessed via Fisher’s exact test, or a chi-square test. Continuous variables were reported as a mean if normally distributed and compared using a T test, or via a median if not normally distributed, and assessed via a Mann–Whitney U statistical test. A two-tailed p value of < 0.05 was considered statistically significant.
Comments (0)