The ability to walk independently without tripping and falling is a significant determinant of the quality of life for individuals with CMT [32]. Patients with CMT have an increased risk of non-osteoporotic fractures, primarily occurring in ankle, hand, or foot [33]. Additionally, the risk of falls may be increased by symptoms and signs such as hand cramps, muscle cramps, difficult walking, and weakness. Therefore, it is crucial to assess the risk of falling to implement orthoses and/or aids, thereby mitigating the risk of fractures and complications due to immobilization. In this scenario, the availability of objective OM of gait function sensitive enough to capture changes in the clinical picture without ceiling or floor effects is crucial. Understanding current therapeutic treatment needs, disease progression, patients’ perception of the disease course, and demonstrating the effects of tested interventions reflecting changes in everyday function is one of the research main topics. In fact, recently, there has been considerable international effort to address this, leading to the conclusion that OM should be carefully chosen r to prove the efficacy of a treatment. A poorly designed study using insensitive OM will fail to demonstrate the effectiveness of a treatment or may lead to improperly positive results. In rehabilitation, increasing importance is being placed on instrumental systems that can capture patient performance quickly and objectively. The GAITRite system seems to be sensitive in discriminating between healthy and pathological subjects and in rapidly assessing walking performances during outpatient visits [34,35,36], even in CMT. As previously mentioned, we chose to investigate the most used spatio-temporal parameters, and we found that in CMT subjects, the most significant parameter is stride length. This data aligns with literature: stride length in our sample is significantly reduced in all tasks compared to healthy subjects, which may be explained by the presence of drop foot or push-off deficits often seen in CMT patients [19]. Multiple factors may contribute to shorter steps. In literature, several studies on children have examined this phenomenon. Particularly, some authors found that the subgroup with the most severe impairment in foot drop and push-off deficit walked significantly slower [18, 37].
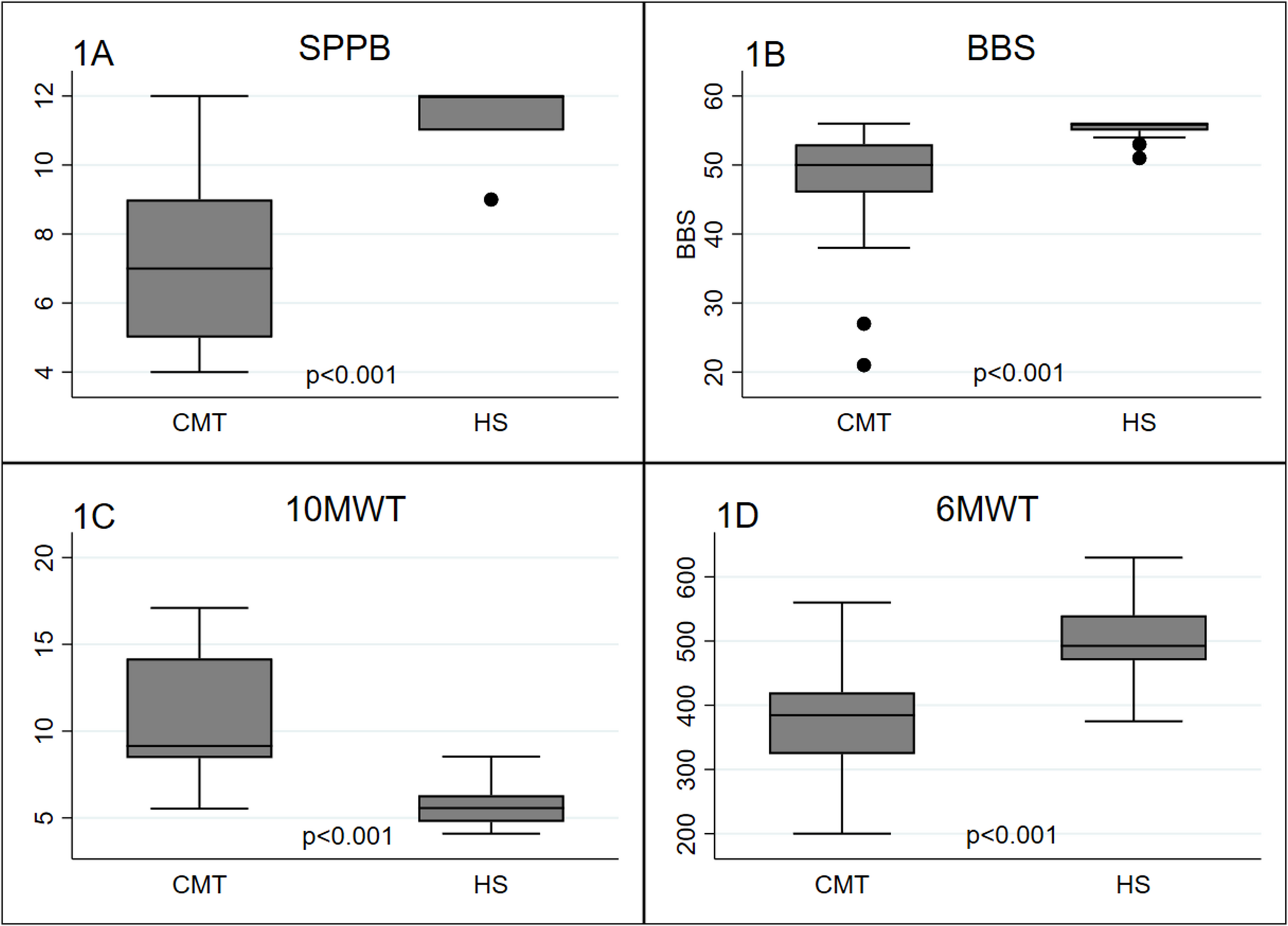
The fact that in this pilot study CMT subjects, despite having a mild to moderate impairment at the CMTES, exhibit significantly worse performances compared to the healthy control group, is not surprising, as gait and balance disturbances are among the earliest to manifest and characterize most subtypes of CMT. The median score of 50 on the BBS, indicating a low risk of falls, and the score of 7 on the SPPB, suggesting a moderate risk of falls, may indicate that SPPB scale is more sensitive to capture imbalance; this impression is reinforced by the evidence of the high significant correlation between SPPB and 6MWT, as the latter has already been recognized as a useful test for assessing the gait of these patients [15, 16].
Furthermore, the fact that the 10MWT, the 6MWT, the BBS, and the SPPB are correlated with each other confirms what is already known, as these are useful OM in assessing CMT patients [15].
In our sample, velocity is reduced in CMT subjects only in NW. Gait speed has been suggested as a predictor of functional change in children with CMT [38]; as previously mentioned, speed may be influenced by reduced step length, foot drop during the swing phase with reduced calf power at push-off, and reduced cadence. The non-significance of the data in the other tasks could be related to the small sample size.
The width of the support base does not appear to be increased in our population of individuals with CMT, which is unexpected, as disto-proximal impairment in motor and sensory functions could lead to a wider base of support to prevent imbalance and falls [30]. However, it should be noted that a greater variability of step-to-step base of support in children with CMT has been described compared to the control group [39].
Regarding the percentage of gait phases, we observed a difference only in stance and swing phases in both FW and DT, with a tendency toward significance in NW. We may suggest that since CMT patients have strength deficits and foot deformities with reduced ankle-foot range of motion, these characteristics are more prominently reflected in the stance and swing phases than in other gait cycle phases. Indeed, the imbalance and gait disorder may manifest as shorter steps with reduced swing phase and prolonged stance. The fact that these parameters show only a trend toward significance in NW may be attributed to the small number of recruited subjects.
We also analyzed the possible correlations between clinical and instrumental OM, finding that the SPPB and the 6MWT present the most relevant correlations with all spatio-temporal parameters. This confirms that these scales are capable of discriminating CMT subjects at risk for falls [14, 15] and may be used in current clinical practice. They particularly correlate with stride length, gait speed, and stride width. As for the percentage of gait phases, we observed a correlation only in stance and swing phases in FW and DT, with a trend toward significance in NW.
In conclusion, even with the limited number of participants with various CMT subtypes, we propose that GAITRite could be an effective tool for assessing the walking patterns of CMT patients, as it appears to distinguish CMT subjects from healthy controls. Additionally, the differences detected with GAITRite are consistent with those reported in literature describing the gait features of patients affected by CMT [18, 37, 40], such as stride length and gait speed.
This could also be valuable in CMT longitudinal assessments, aligning with established OM. Nonetheless, these correlations need validation with a larger sample. Future studies should include longer periods for gait assessment. Understanding gait disorders better in CMT patients could lead to tailor-made rehabilitation protocols, enhancing healthcare and quality of life.



Comments (0)