
Remember me






The patient was a 54-year-old male who initially developed heart failure at the age of 40 and was diagnosed with dilated cardiomyopathy. A myocardial biopsy was conducted and a diagnosis of idiopathic dilated cardiomyopathy was made. The patient was treated with angiotensin-converting enzyme (ACE) inhibitor, beta-blocker, and sacubitril valsartan. The patient continued the treatment thereafter. At the age of 54, he experienced respiratory distress, leading him to seek medical attention and subsequent hospitalization with the diagnosis of acute exacerbation of chronic heart failure. Catecholamines were administered to treat heart failure. During hospitalization, the patient experienced cardiac arrest and underwent cardiopulmonary resuscitation, including chest compressions, which resulted in the restoration of cardiac activity. Coronary angiography was performed, but there was no significant stenosis, and the cause of cardiac arrest was unknown. Venoarterial extracorporeal membrane oxygenation (VA-ECMO) and intra-aortic balloon pump (IABP) were initiated, and the patient was subsequently transferred to our hospital for multidisciplinary treatment. VA-ECMO was established by securing a blood supply channel from the right femoral artery and a debridement channel from the right femoral vein. Echocardiography revealed an ejection fraction (EF) of 26%, a left ventricular end-diastolic diameter (LVDD) of 64 mm, and severe mitral regurgitation (MR) (Fig. 1A, B). Gradual recovery of cardiac function was observed, and ECMO was discontinued on the third day after transfer. On the fifth day after transfer, the patient developed hypotension. Contrast-enhanced computed tomography (CT) revealed bleeding from the thymus and a significant hematoma in the mediastinum (Fig. 2A, B). An emergency sternotomy was performed for thymic hemostasis and hematoma removal. Subsequently, catecholamine support was discontinued and the patient was weaned off the ventilator. For residual severe MR, transcatheter mitral valve repair was performed on the 84th day after transfer. The mechanism of mitral valve regurgitation in this case was primarily due to the tethering caused by left ventricular dilation and mitral annular enlargement, which is often a result of idiopathic dilated cardiomyopathy. The placement of a single MitraClip successfully controlled the mitral regurgitation. The patient was discharged ambulatory to home on the 92nd postoperative day. One month later, the cardiac resynchronization therapy defibrillator (CRT-D) was implanted. Although a screw-type atrial lead was initially placed, it was repositioned to the free wall of the left atrium because of poor electrical potentials and thresholds in the right atrial appendage (Fig. 3). Three months after CRT-D insertion, the patient was transported to our hospital by ambulance because of hypotension. Contrast-enhanced CT revealed a pericardial effusion of approximately 20 mm adjacent to the posterior wall of the left ventricle (Fig. 4), leading to a diagnosis of cardiac tamponade. Emergency left fourth intercostal mini-thoracotomy was performed for pericardial drainage, and a drain was placed. Upon returning to the ICU, 1200 mL of bleeding was observed from the drain, necessitating a median sternotomy in the operating room. In the previous surgery, the pericardium was not opened because of bleeding from the thymus tissue. When reopening the chest, we were careful to avoid damage to the unnamed vein, and there was no adhesion in the pericardial sac. The pacemaker lead was exposed approximately 1 mm from the left side of the right atrium, likely causing chronic abrasion of the aorta (Fig. 5). Bleeding from the ascending aorta was observed and was subsequently controlled. The hole was closed with 4-0 prolene thread with pledget and hemostasis was achieved. Although the lead screw had protruded from the right atrium, there was no bleeding from the atrium itself. We determined that attempting to re-position the lead could significantly extend the surgical time, thereby increasing the overall invasiveness of the procedure. As a result, our strategy during this operation was to focus solely on hemostasis without attempting to re-position the lead. The protruding area of the right atrial lead was covered with biological glue and the chest was closed. As the surgical procedure progressed, hemostasis was achieved, and before closing the chest, the functionality of the defibrillator was checked, and no issues were observed. Subsequent recovery was uneventful, and the patient was discharged on the 18th postoperative day.
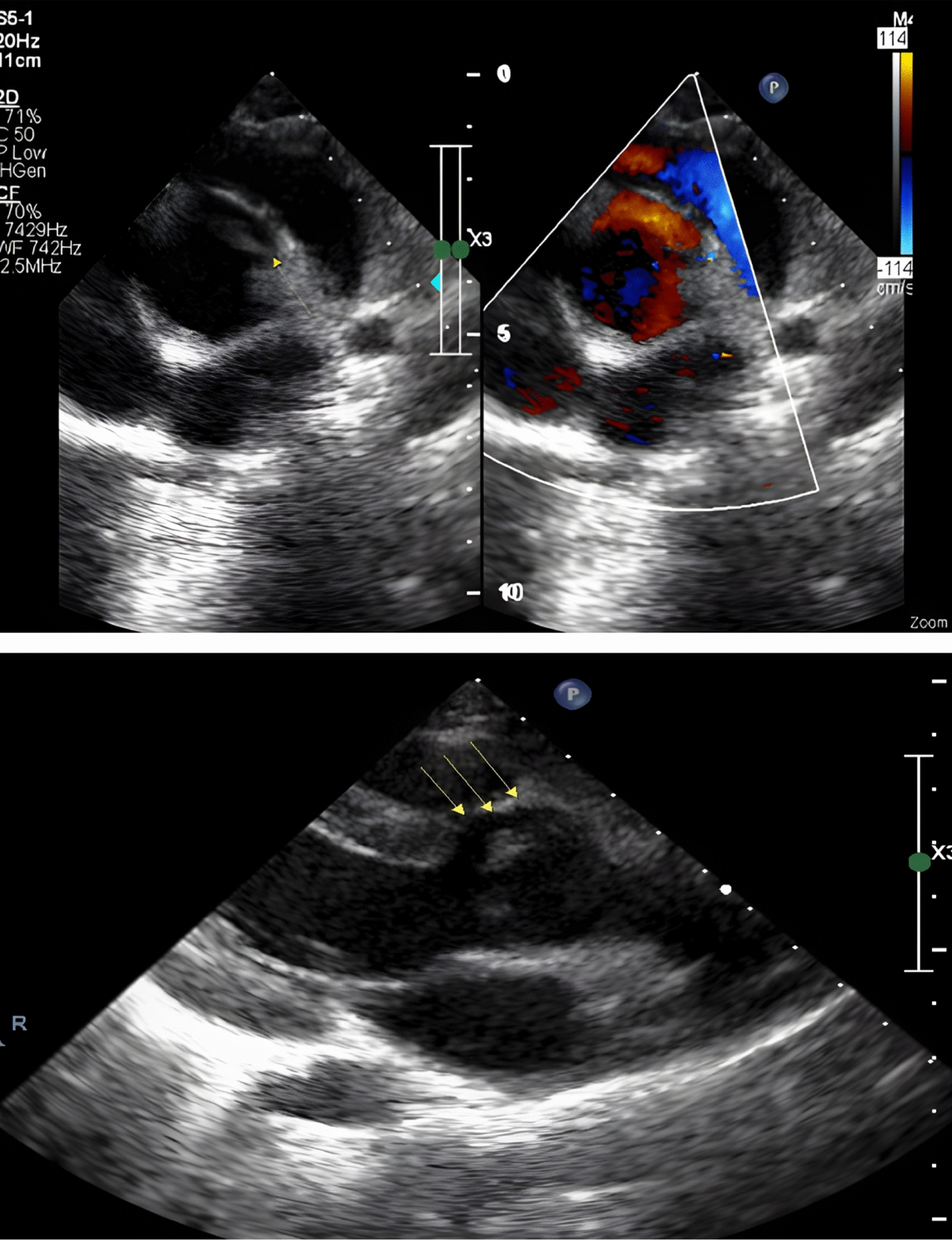
Fig. 1
Preoperative echocardiogram. A Biplane mode of early systolic phase. B Severe mitral valve regurgitation was detected
Fig. 2
Preoperative images of enhanced computed tomography. A Axial view and B coronal view. Venous hemorrhage from the thymus gland was noted (green arrow)
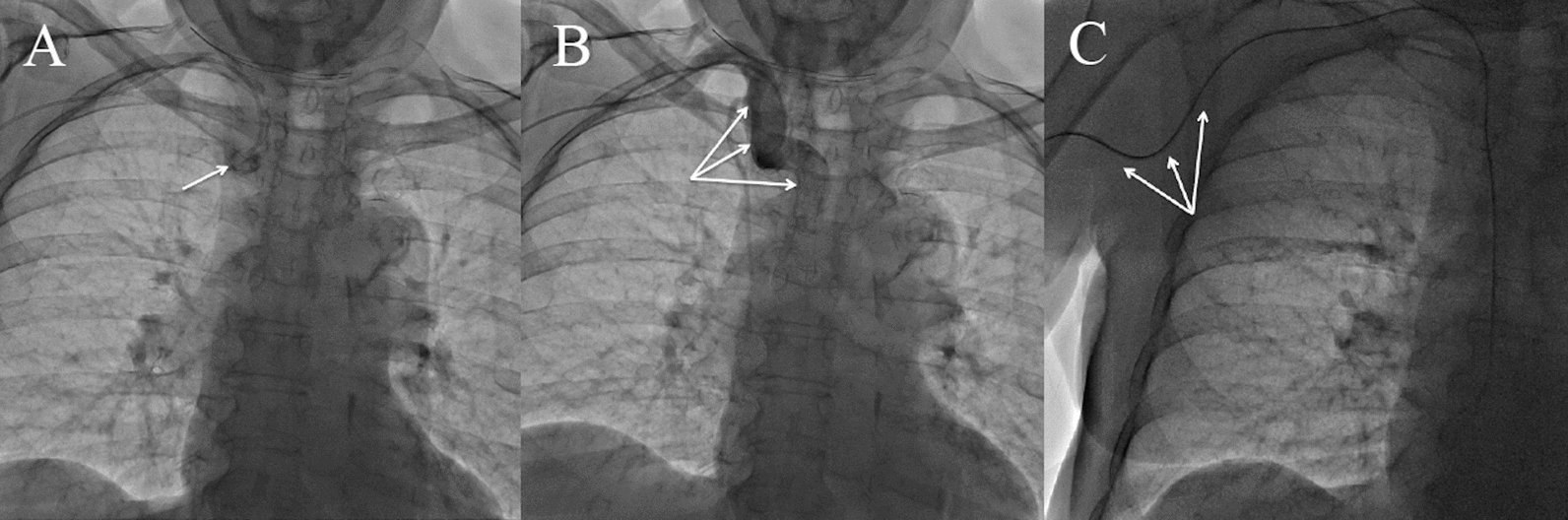
Fig. 3
Postoperative chest radiograph after cardiac resynchronization therapy-defibrillator placement
Fig. 4
Preoperative computed tomography image to evaluate for cardiogenic shock. A 20-mm pericardial effusion was observed posterior to the left ventricular wall. The atrial lead tip was located proximal to the ascending aorta (green arrow)
Fig. 5
A Intraoperative schema. A 2-mm-sized hole was observed in the ascending aorta relative to the tip of an atrial lead penetrating from the right atrium. B Right atrium with a pledget to cover the pacemaker lead
Comments (0)